Breast and Chest Veins
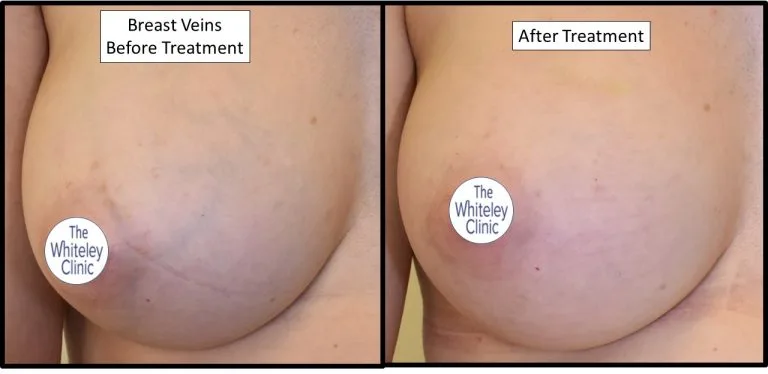
Removal of breast veins before and after at The Whiteley Clinic – Pioneering Vein Treatments
Prominent or unsightly veins on the breast or chest can be very distressing. They are usually a green colour and are frequent enlarged and bulging. Bulging depends on position and temperature. When sitting or standing they often look worse – and of course heat makes them dilate.
It is usually a problem in women after puberty who have developed a female breast. However, in some conditions, men or girls before puberty can develop prominent veins.
We will discuss these less common cases later. For now, we will concentrate on breast veins and chest veins in the adult female.
Who gets prominent breast veins and chest veins?
There are no definite statistics as to how many women suffer with prominent breast veins. One research paper did look at women before and after breast implants. In a fairly small sample of 78 patients, they noted that:
- 44% of women had prominent breast veins before breast implants
- 96% of women had prominent breast veins after breast implants
Thus, it would appear that women can have prominent breast veins naturally. However, after breast implants, it appears that the majority of women will develop prominent breast veins.
Which Breast Veins Can Be Treated?
It is unwise to consider any treatment at all in breasts that are still developing. As such, unless there are special circumstances, it is unwise to consider any intervention at all in women under 18 years old.
Also, as hormone changes can change the size and prominence of breast veins and chest veins, no-one should consider any treatment if they are pregnant, breast feeding or the first 3 months after pregnancy or stopping breast feeding.
Similarly, if the veins have only appeared since taking the oral contraceptive pill or hormone replacement therapy, then care should be taken before thinking of any intervention. These veins might go of their own accord when the hormones change again.
Therefore, veins that are large, unsightly and/or prominent on the breasts or chest in women over 18 years, who are not pregnant and whose veins have not suddenly changed, are most likely to be suitable for treatment. Women who have had breast implants are even more likely to have breast veins suitable for treatment.
Removal of Breast Veins
Unlike veins of the legs and pelvis, breast veins and chest veins do not have underlying veins feeding high pressure blood into them.
Therefore, there is not usually any need for a duplex ultrasound or any other scan of the veins. This is one of the few areas in phlebology where the assessment of the veins can be made safely without a duplex ultrasound scan or other test. However, do note the few exceptions to this noted below.
However, although there is no link between prominent breast veins and breast cancer, if there are any concerns at all about any lumps in the breast, nipple discharge, any sudden change in the breast veins such as the veins suddenly going hard and red (thrombophlebitis or clots of the breast veins), or indeed any worries about the breast itself, it is best to see a breast specialist first to ensure the breast is healthy.
Prominent or enlarged breast veins and chest veins can be treated by a special form of “phlebectomy”. Phlebectomy literally means vein (phleb….) removal (….ectomy).
Prof Mark Whiteley has developed and method of performing an aesthetic phlebectomy of the breast veins and chest veins under local anesthetic only. He and his team use a special incision technique and instruments that reduce the risk of scars over the usual incisions that are made in the skin.
The incisions are so small, no stitches are needed. In fact, the wounds are closed using a small amount of tissue glue only. When this glue falls off, the incisions are healed and are fast disappearing.
Foam Sclerotherapy Treatment for Breast Veins or Chest Veins.
Injecting sclerotherapy as a foam can be very effective in treating smaller and flatter veins of the breast and chest.
Veins that are blue or green, and that are quite narrow and do not bulge, tend to be the ones that respond best to foam sclerotherapy.
If the vein is too large or prominent, then it is more likely that foam sclerotherapy will cause a clot in the vein and a brown mark that might stay for a long time – or rarely might be permanent.
Therefore, we only recommend foam sclerotherapy for small and non-bulging veins on the breast and chest.
In addition, we recommend patients to wear very strong support for 3 weeks day and night over the areas of foam sclerotherapy injection to get the best results and lowest risk of brown stains.
Depending on the extent of the breast veins, more than one session of foam sclerotherapy might be needed.
We recommend waiting at least 8-12 weeks after each treatment before assessing the result and deciding if any further treatment might be needed.
Combined Treatment for Breast Veins and Chest Veins
Some patients, especially those who have had breast implants, can have very extensive breast veins of varying sizes.
In such patients, we often start with aesthetic phlebectomy and then wait 8-12 weeks to see the results.
If small blue / green veins remain, we can then start foam sclerotherapy treatment. Once again, we then wait for 8 – 12 weeks to see if any further treatment might be needed.
Use of Ultrasound in Breast Vein Treatment:
Although I have noted above that we do not “need” duplex ultrasound to assess or treat breast veins, there are a few exceptions where we do need to do so.
- Assessment of depth of implant: in patients with breast implants, it can be necessary to measure how deep the implant is under the skin. When planning aesthetic phlebectomy or foam sclerotherapy, it is important that any needles or sharp instruments are kept well away from the implant.
- Guiding foam sclerotherapy: on occasion, the vein to be treated is so small that it is necessary to use ultrasound to guide the injection directly into the correct vein.
- Checking for thrombophlebitis in breast vein: If there is any suggestion that the vein might have become inflamed or have clotted, a duplex scan will show if there is clot in the vein or if it is open and flowing normally
- Checking for underlying conditions such as axillary (arm-pit vein DVT): in rare cases when the distribution of veins looks abnormal, a duplex ultrasound scan can be used to see if there is an underlying problem. Rarely there can be a deep vein thrombosis (DVT) of the axillary vein (the vein in the armpit). This can cause a lot of veins to appear over the shoulder and one side of the chest. There are also other even rarer conditions such as abnormalities of veins and arteries that can appear on the breast or chest that might need further investigation.
Results
There is no objective measure of “cure” because breast veins and chest veins is an aesthetic (cosmetic) condition. Therefore, it is current impossible to “measure” success objectively.
However, that being said, our experience to date is a very high level of patient satisfaction with breast vein and chest vein treatment.
We will be publishing our results in due course but to date, we have not had any patients who have not had a good to excellent improvement in their treated breast veins or chest veins.
What to do now:
If you have breast veins or chest veins that you want to have removed, you can contact us to arrange an appointment with one of our specialist consultants.
If you have any questions, or are unsure in any way about your condition, you are welcome to contact us. Our staff will be able to answer most questions and, if your question is clinical and about your medical condition, one of our consultant specialists will be able to advise you.
Reference