Pelvic Congestion Syndrome (PCS)
The symptoms of PCS predominantly come from the weight of the blood pushing on these structures.
It is not known exactly what proportion of females suffer from pelvic congestion syndrome. However, in the past, many gynaecological texts have estimated that up to a third of patients in gynaecology outpatients do not have anything wrong with them with relation to the gynaecological conditions that are readily investigated. However pelvic congestion syndrome is rarely checked for by gynaecologists and a surprising number of gynaecologists report ‘large varicose veins in the pelvis’ at investigation such as laparoscopy, even though they then say that the test was normal.
It is becoming evident that because gynaecologists have not been brought up to diagnose this condition, a great many women who are suffering from the symptoms of PCS are not having the appropriate investigations (transvaginal duplex ultrasound scan) but are instead being put through expensive and needless tests such as MRI, CT and even laparoscopy under general anaesthetic and then being told that there is nothing wrong with them!
As leading research centres such as The Whiteley Clinic improve the understanding of venous conditions, particularly pelvic venous problems, more and more patients should get properly diagnosed and treated rather than palmed off as ‘being normal’ by doctors who do not specialise in pelvic venous conditions.
Background of the term ‘pelvic venous congestion’
As with most names in medicine, the term “pelvic venous congestion” is really just a description of the problem:
- ‘Pelvic’ – means that it relates to a condition of the pelvis
- ‘Congestion’ – meaning too much blood in the veins and hence the venous circulation is “congested”
- ‘Syndrome’ – means a collection of different symptoms and signs
The Whiteley Clinic and referrals
The Whiteley Clinic is a specialist unit and is a private medical facility. We encourage you to get a referral from your general practitioner although if you do not wish to do so, we will still see you without one.
Causes of Pelvic Congestion Syndrome
Similarly, with all varicose veins, the underlying cause of pelvic congestion syndrome are when the pelvic vein valves fail.
As outlined in the introduction, pelvic congestion syndrome is the name given to the condition caused by swollen varicose veins in the female pelvis. Due to the male anatomy, it is rare in males although males can get problems with pelvic vein incompetence including varicoceles, haemorrhoids, leg varicose veins and even impotence. However male pelvic vein problems are a very specialised area that will be discussed elsewhere.
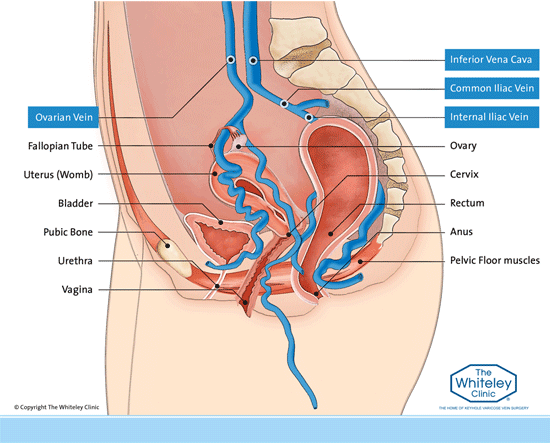
In females, there are four major veins involved in pelvic congestion syndrome. These are the right and left ovarian veins and the right and left internal iliac veins.
As with all veins, in the normal situation blood is pumped up the veins towards the heart. In the very large veins such as the common iliac vein and the inferior vena cava, there is fairly continuous flow and so valves are not needed and so do not usually appear. However in the internal iliac veins draining blood from the anus, perineum, vulval and vagina and also in the ovarian veins, draining blood from the ovaries and uterus, the flow is slow enough to require valves to be present.
Similarly, with all varicose veins, the underlying cause of the pelvic varicose veins are when these valves fail. The valves can fail in 1, 2, 3 or 4 of these veins causing blood to fall the wrong way down the veins (pelvic venous reflux) and causing the veins lower down to dilate (varicose veins).
Because the ovarian veins are long, they are easier to see on scanning and easier to treat and so a lot of doctors and clinics concentrate on ovarian vein reflux only. However research published in peer review journals from The Whiteley Clinic has shown that only 3% of women with pelvic venous reflux have only ovarian vein reflux and the commonest pattern of pelvic vein reflux is left ovarian vein and both internal iliac veins. Hence those concentrating on only the ovarian veins will be missing the vast majority of patients with pelvic venous reflux.
The pelvic venous reflux occurs passively when standing or sitting, as the blood falls back down the veins due to gravity. When the woman lies flat, gravity then helps the blood return to the heart normally and so the symptoms of pelvic congestion syndrome improve. This is improved further still if the woman lies down on a slope up, with her bottom raised above her chest.
This is also a reasonably good way to check whether pelvic symptoms might be due to pelvic congestion syndrome. If the symptoms worsened during the day when the patient is up and about, but improve after a night’s sleep in bed, then pelvic congestion syndrome is much more likely.
Who gets symptoms from Pelvic Congestion Syndrome?
Pelvic congestion syndrome (PCS) affects women in their childbearing years. It is uncommon for girls to get pelvic congestion syndrome before puberty, as the pelvic organs and blood supply have not increased due to the effect of female hormones. Similarly, it is uncommon to get pelvic congestion syndrome after menopause, as when the female sex hormones reduce sufficiently, the blood supply to the pelvis also reduces. However, it is possible to get pelvic congestion syndrome postmenopausally if the veins have been very dilated.
What are the symptoms of PCS?
The symptoms of pelvic congestion syndrome are mainly those caused by the pressure of the venous blood in the dilated pelvic varicose veins pressing on the pelvic organs. As such they can include:
- aching or dragging feeling in the pelvis, particularly on standing. This is due to the weight of blood in the pelvic varicose veins weighing heavily on the pelvic floor which is made of muscle. It is usually worse around the time of the period
- irritable bladder sometimes giving stress incontinence, due to the weight of the pelvic varicose veins on the bladder
- irritable bowel due to the weight of the pelvic varicose veins on the rectum
- discomfort on sexual intercourse medically referred to as ‘deep dyspareunia’
Although there are rarely any outward signs of pcs, occasionally the following can be seen, particularly after pregnancy:
- varicose veins of the vulval or vagina (bulging veins around the front passage). Often these are visible during pregnancy and look as if they have disappeared after delivery. However this is just because they have got smaller. The underlying venous reflux is usually still there
- small varicose veins visible at the top of the inner thigh next to the vulva but on the leg, or the backs of the thighs usually around the buttock crease, anus or perineum.
How do I know if I have PCS?
Unfortunately many of the symptoms of pelvic congestion syndrome are variable and also can occur with other conditions. Usually patients come to The Whiteley Clinic once they have already seen their family doctors and gynaecologists and have been told that there is nothing wrong with them.
Research performed at The Whiteley Clinic and published in peer-reviewed journals has suggested that the best way to diagnose varicose veins of the pelvis is a specialised venous duplex ultrasound test called the transvaginal duplex ultrasound. Judy Holdstock and Charmaine Harrison, the two most senior vascular technologists at The Whiteley Clinic, have developed the Holdstock-Harrison protocol to diagnose pelvic vein reflux and pelvic varicose veins.
The research suggests that this is more accurate than MRI, CT, venography or any other test that is used currently.
One of the major advantages of transvaginal duplex ultrasound is that the ovaries, uterus and cervix can also be examined at the same time using a test that has no x-rays and has no needles at all and is a truly walk in walk out investigation.
PVE – Pelvic Congestion Syndrome Treatment
Pelvic Vein Embolisation (PVE) is safe, effective at stopping the pelvic vein reflux and gives long-lasting results!
The Whiteley Clinic started treating pelvic vein reflux (PVR), the underlying cause of pelvic congestion syndrome (PCS), in 1999. It was one of the first clinics in the world to start treating this condition and indeed there are now considerable numbers of publications in the peer-reviewed medical literature from The Whiteley Clinic.
Recent research from The Whiteley Clinic has shown that the treatment used, pelvic vein embolisation (PVE) is safe, effective at stopping the pelvic vein reflux and gives long-lasting results.
Pelvic Vein Embolisation (PVE)
Unlike the veins of the leg, which are surrounded by subcutaneous fat, the pelvic veins have got very sensitive organs and vital structures around them. As such, we cannot use the heat-producing method such as laser, which might end up burning the ovaries, uterus, vagina, bowel, bladder or indeed the ureters, nerves or arteries. Therefore to be able to treat these veins successfully, we need to be able to close them without using heat.
Open surgery or laparoscopic surgery is not particularly useful to treat pelvic veins. Firstly, the pain and complications from open surgery is not needed. Secondly, it is exceptionally difficult to get to the very small veins involved deep in the pelvis by using open surgery or laparoscopy.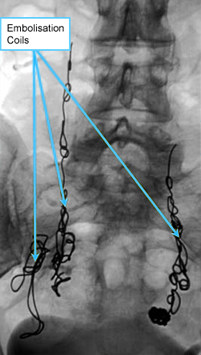
By using x-ray guided venography, planned by the results of the transvaginal duplex ultrasound, we are able to place very thin catheters directly into the veins that need treatment. Once the catheter is in place, a combination of foam sclerotherapy and insertion of a specialist inert metal coil can be placed into the vein, closing it and stopping the pelvic vein reflux.
Like our other treatments, PVE is performed under local anaesthetic as a walk-in, walk-out treatment at The Whiteley Clinic, Bond Street, London.
Although some patients are concerned about having coils placed into their pelvic veins, the actual metal involved is less than the clips used in many surgical procedures such as laparoscopic hernia repair or laparoscopic gallbladder removal and far far less than the metal used in a hip replacement or other joint replacement procedure.
Our published research has shown this to be a highly effective technique with exceptionally low complication risks even in the long term.
However, there are very few centres in the world that have a big experience of with these procedures, particularly in the internal iliac veins which are more usually the problem than ovarian veins.
The Impact of Pelvic Congestion Syndrome
We worked with PB Consulting and Boston Scientific to investigate the impact of Pelvic Congestion Syndrome (PCS) in the UK.
As part of this report, almost 100 women were surveyed. On average the respondents had 16 GP appointments before diagnosis and some patients had as many as 13 diagnostic tests during the 4 years it took for them to be correctly diagnosed.
A Freedom of Information request was sent to all 154 NHS Hospital Trusts in the UK and shockingly only 5 trusts said that they offered a specific test for Pelvic Congestion Syndrome.
Past Patient’s Perspective

Lindsey Lockett has been symptom free since her pelvic vein embolisation at The Whiteley Clinic in London in 2019
For more information from a past patient’s perspective on Pelvic Vein Embolisation and Pelvic Congestion Syndrome please contact Lindsey Lockett.
Lindsey, who resides in America, was diagnosed with PCS in 2018 and underwent her treatment at The Whiteley Clinic in London in mid-2019. Lindsey has documented numerous blog posts on the condition as well as her treatment.