Vulval & Vaginal Varicose Veins
These veins usually appear in pregnancy and then ease a little after child-birth – although once they have come they do not go completely. Further pregnancies worsen the condition.

In some women the varicose veins stay in the vulva – in many they lead to varicose veins in the top of the thigh – on the inner part of the leg (next to the vulva). These can then lead to varicose veins down the inner part of the thigh or can lead to veins down the back of the thigh.
Most doctors or surgeons do not currently look for this condition and do not know that there is an effective treatment for this. There are some companies that sell “supports” for the vulval varicose veins – however such devices only provide some support and do not get to the root cause of the problem – pelvic vein reflux (or ovarian vein reflux).
Most doctors or surgeons who treat varicose veins either do not know about this condition or do not treat it. As such most either ignore it, or just “pull the veins out” of the top of the thigh – or even inject them. This gets rid of the veins in the short term, but as it does not get rid of the cause of the veins, they come back very soon afterwards.
Here at The Whiteley Clinic we have been studying this problem since 1999 and have developed a process of recognising the problem, identifying the exact cause and then treating it effectively, using the latest non-invasive diagnostic techniques and minimally invasive treatments. It requires a team approach of Vascular Surgeon, Vascular Scientist and Interventional Radiologist.
The techniques that we use are well recognised, tried and tested – we have developed a protocol based approach that is proving very successful in treating this condition.
Professor Whiteley and the members of The Whiteley Clinic have already published research on this subject and more research is on the way to show the effectiveness of their treatment.
Symptoms of Vaginal & Vulval Varicose Veins
The distended veins around the ovary and in the pelvis can push on the bladder and rectum. This can give symptoms of:
- Pelvic Pain or Aching
- Dragging Pain in Pelvis
- Stress Incontinence worsened
- Irritable Bowel Syndrome worsened
As the hormones in the menstrual cycle affect these veins, these symptoms (if present) are worse around the time of the period.
Not every woman with pelvic vein reflux gets symptoms. Many don’t know there is any thing wrong UNTIL they get pregnant.
During pregnancy the veins in the pelvis dilate further – and then open up varicose veins in the vagina – then the vulva – and finally into the legs.
Women with this problem seem to develop vulval varicose veins and vaginal varicose veins during pregnancy (we have found two ladies with this condition who haven’t been pregnant).
When the baby is delivered, the vulval varicose veins and vaginal varicose veins usually get smaller as the hormones reduce.
However, the veins that have been opened have lost their valves and hence continue to reflux. If left untreated, these veins spread into the leg and appear as varicose veins.
In some women the veins have been so distended, they can’t return to normal afterwards and they remain with large, unsightly and occasionally painful varicose veins of the vulva and vagina.
These problems can all be cured using the techniques that we have developed at The Whiteley Clinic.
Vulval and Vaginal Varicose Veins Treatment
Up until the year 2000 we had looked at several different Vulval & Vaginal Varicose Veins treatments- but all of these older methods had major drawbacks or high failure rates. We had tried operating directly on the veins in the pelvis either by open surgery or by Laparoscopic (keyhole) surgery – but these approaches had been traumatic to the patients and had given fairly poor results.
In colaboration with several experts, we decided the best way forwards was to use “Coil Embolisation”. This is an x-ray technique where a needle is put into a vein – and under x-ray control, a thin tube called a catheter is pushed into the vein you wish to treat. When it is the correct place, a metal “coil” is pushed out into the vein.
These coils are not new – they have been used for over 20 years in different areas of the body to block off blood vessels, so we know them to be safe and effective.
For many years they have been used to block off male testicular veins – in the treatment of varicoceles – and there is a lot of experience from some specialist centres over several years in using these in ovarian veins. However, it is not just the coil embolisation that is important – it is how it is done. The coils are placed in position by an interventional radiologist under X-ray control. Most interventional radiology is performed via the groin.
Tests for Vulval & Vaginal Varicose Veins
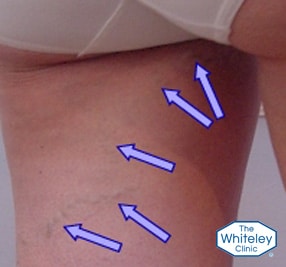
The first way to diagnose this problem is by simply looking. Usually there is a history of Vulval Varicose veins in pregnancy. Looking at the top of the thigh, there is a Tendon called the Adductor Longus tendon.
This can be easily felt in everyone – it feels hard and like a tube to the touch. If the veins arise in front of this tendon, then they almost always come from the veins in the legs – these are NORMAL varicose veins.
If the veins arise behind this tendon (see picture on right), on the inside of the thigh – or running down the back of the leg, then they are almost always coming from Ovarian or Pelvic veins reflux. These veins cannot be treated by traditional methods of varicose vein surgery.
Trans-vaginal Duplex Ultrasound (TVS)
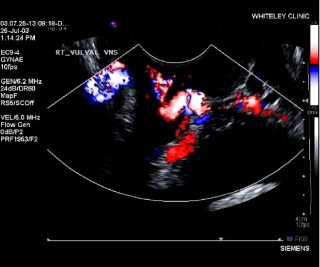
When ovarian or pelvic vein reflux is suspected, or vulval varicose veins have been seen, or when varicose veins appear in the legs behind the Adductor Longus tendon, a specialised Ultrasound examination is required.
The veins in the pelvis cannot be seen easily by ultrasound across the abdomen – as they are too deep.
Therefore, we use a special ultrasound probe that can see the veins through the vagina.
Our specialist female vascular scientists perform this test and can check if there are varicose veins in the pelvis – and if there are – where they are coming from.
Although most do come from the ovarian veins (as described before) there are other veins in the female pelvis that can also cause the same thing – the internal iliac veins.
The scientists can show the patient what is happening as they carry out the scan – and then they write a detailed report so that the consultants can try to plan appropriate treatment.
These problems can all be cured using the techniques that we have developed at The Whiteley Clinic.
Ovarian Veins in Women
The ovaries are the female gonad – the equivalent to the male testicle. Before birth the ovaries grow in the same place in the foetus – up by the kidney. As the baby girl develops, the ovaries move down into the pelvis – taking their veins – the ovarian veins – with them.
This is identical to the male – with the sole exception that the ovaries stay inside the pelvis and do not continue to the outside, as the testicles do.
Not surprisingly, the ovarian veins can go wrong just as the testicular veins can.
In exactly the same way, if the valves in the ovarian vein give up working, a “varicocele” is formed around the ovary.
Ovarian, or Pelvic, Varicocele – ‘Varicose Veins in the pelvis’
Again, not surprisingly the swollen veins in the pelvis can cause aching and a “dragging” feeling, especially during a period – just as a variocele around a testicle can cause symptoms.
However, there are 2 main differences in women:
Firstly, the veins can spread further in the pelvis, pushing on the bladder and bowel and irritating them.
Secondly, as they are on the inside and therefore invisible to doctors, they are usually ignored by doctors and patients alike – the symptoms being put down to “women’s problems”.
Clinical grading scale for varicose veins of the vulva – The Whiteley Clinic grading scale
Whenever medical people need to communicate with each other or decide on treatments, it is very useful to have a recognise grading scale for the condition.
Before 2012, there was no clinical grading scale in use for Vaginal and Vulval Varicose Veins.
In early 2012, the following grading scale was published by The Whiteley Clinic, and is now used to classify the severity of any patients presenting with varicose veins of vulva:
- Grade 0 – Normal
No vulval varicosities and no venous reflux are present.
Frequency: Usual - Grade 1 – Venous reflux without visible vulval varicosities
No visible varicose veins in the vulva; however, ultrasound confirms reflux in the vulval veins.
This is usually associated with para-vulval varicose veins seen on the inner thigh.
Frequency: Common – approximately 1 in 7 women presenting with leg varicose veins (1 in 5 after vaginal delivery) - Grade 2 – Visible vulval varicosities
Varicose veins are visible through the mucosa of the inner labia and lower vagina, with ultrasound-proven reflux in the vulval veins.
Frequency: Uncommon - Grade 3 – Isolated vulval varicosities
Varicose veins are seen on standing through the skin of the outer labia majora, without distortion of the general anatomy of the area.
Frequency: Very uncommon - Grade 4 – Extensive vulval varicosities
Widespread varicose veins of the labia causing distortion of the skin and overall anatomy when standing.
Frequency: Rare