


Varicose vein research laboratory
February 19, 2026
A very fit and healthy 60-year-old lady came to The Whiteley Clinic for a second opinion, having been told that she had left leg lymphoedema.

Swollen left ankle due to hidden varicose veins venous reflux misdiagnosed as lymphoedema
She was told that the treatment was generally manual lymphatic drainage and compression, but new lymphatic operations might be suitable. She had previously had her veins investigated elsewhere and had been told there was nothing major wrong with them. Fortunately, her plastic surgeon asked for a second opinion about her veins from The Whiteley Clinic before he decided whether to proceed with lymphatic surgery. When the lady was first examined, she clearly had swelling of her left ankle and lower leg up to the knee. However she did not have swelling of her toes. Swelling due to leg lymphoedema usually goes into the toes causing the toes to be very swollen. When the swelling is predominately at the ankle, it is often a vein problem - usually venous reflux or "hidden varicose veins" and sometimes obstruction of the veins (such as a May-Thurner syndrome).

Swollen left ankle due to hidden varicose veins venous reflux misdiagnosed as lymphoedema standing
The patient did have some small varicose veins on her calves which had been noted previously. However she had gone to a teaching hospital in London where she underwent an old-fashioned venogram and was told that the veins had no blockages in them. She had a venous duplex ultrasound scan performed elsewhere which suggested that her veins were generally working normally but she might have some small perforators.

Right leg showing small varicose veins only despite Great Saphenous Vein reflux
When she had the examination and then venous duplex ultrasound scan by the The Whiteley Clinic team, it was found that her previous diagnosis was severely in doubt. On the left side, where the ankle was very swollen, there was a massive "hidden varicose vein". This was the great saphenous vein which not only had lost is valves, letting blood fall down the leg causing problems at the ankle, but had dilated to a massive 11 mm in diameter. A normal vein in this sort of lady should be 4 mm in diameter. As the amount of blood passing through a vein is equivalent to the area of the vein, this meant that her dilated vein was in fact 121 mm² (11mm ×11 mm) rather than the normal 16 mm² (4 mm times 4 mm).
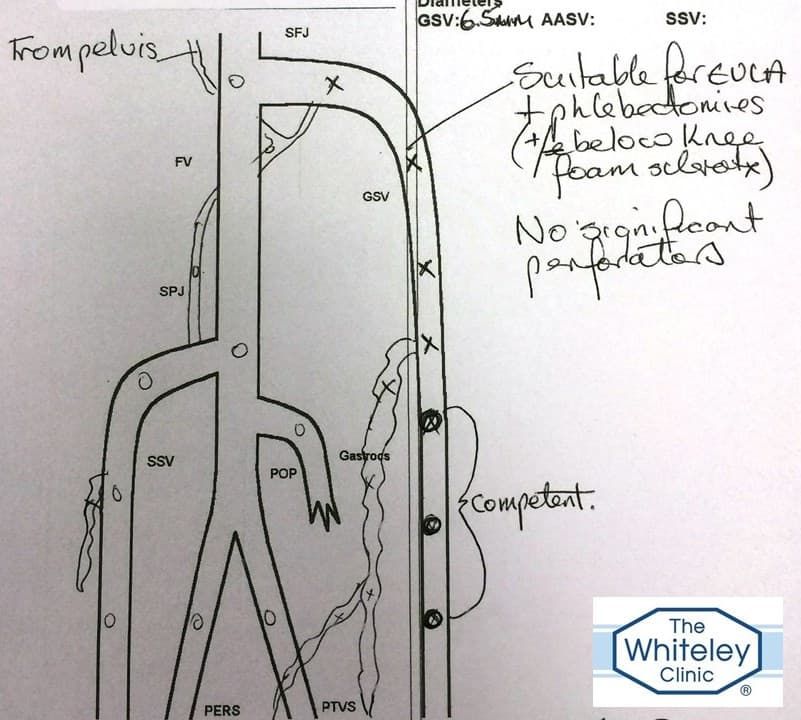
Duplex Ultrasound Report showing hidden varicose veins venous reflux misdiagnosed as lymphoedema
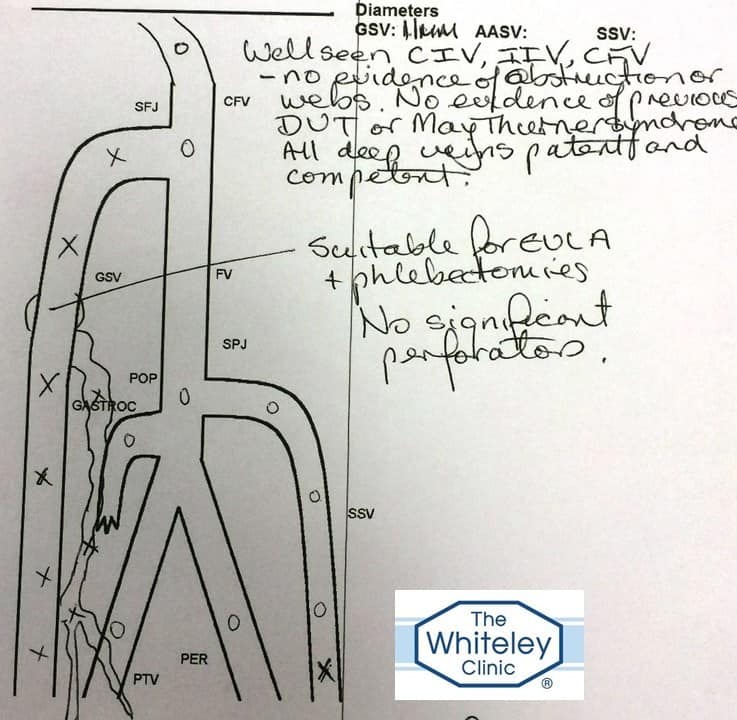
With such a massively dilated vein which was incompetent and allowing blood to reflux down it, it is highly likely that the majority of the swelling of the ankle is due to this "hidden varicose vein". The fact that virtually no varicose veins are visible on the surface, makes the matters worse. Varicose veins that are seen on the surface act as "shock absorbers" reducing the risk of leg swelling and venous ulceration (for a full explanation of this see "Understanding Venous Reflux - the cause of varicose veins and venous leg ulcers"). On the right side, she also has hidden varicose veins but the vein is much smaller at 6.5 mm diameter and the reflux does not reach the ankle, showing why there is not so much swelling on this side. Interestingly she did have some swelling proven on ultrasound although she had not notice this due to the swelling on the left side.
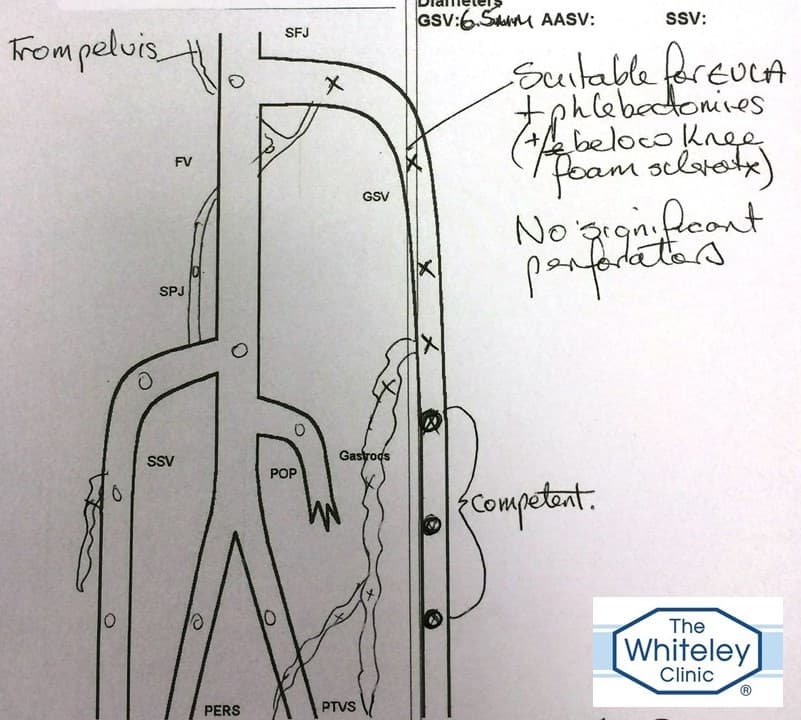
Duplex Ultrasound Report right varicose veins
All of this was explained to the patient and she was offered endovenous laser ablation under local anaesthetic using a 1470 nm laser and the parameters shown by the Whiteley Protocol to be most effective to close such veins. She was warned that this might not get rid of all of the swelling as the may be some lymphoedema present as well as the venous reflux. However, once the venous reflux had been treated with the endovenous laser ablation, the leg would start to recover and after some 3 to 6 months, the swelling should be substantially reduced. In six months time, after she has had treatment as per the Whiteley Protocol and allowed time for the deep venous pump to get back to normal, we will know if she actually needs any lymphoedema treatment at all.