Varicose vein research laboratory
February 19, 2026
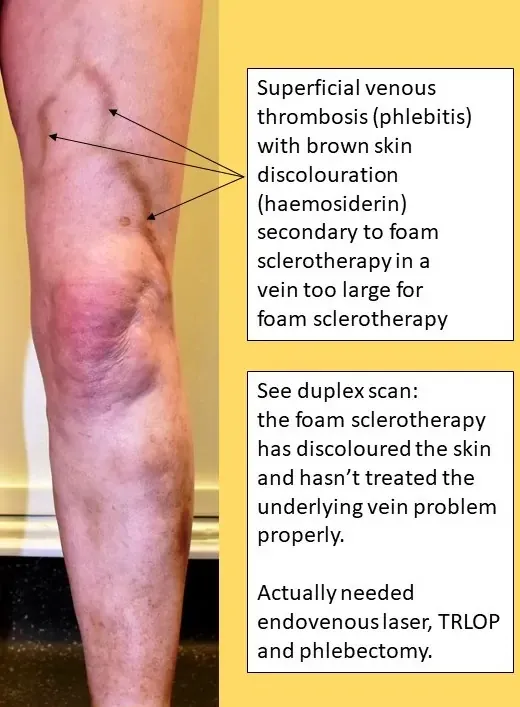
Patients are often told they have "cosmetic" varicose veins by non-specialist doctors or nurses. Or patients might be told that the problem is "only varicose veins". This 58-year-old gentleman came to The Whiteley Clinic with a right sided leg ulcer. The last 20 years he has been going to his GP for his varicose veins. The varicose veins had not been painful. Nor had they caused any aching, itching or other symptoms. Because of this, over 20 years the GP told him that he "only had varicose veins" and these didn't need treatment. As they "didn't hurt" they were "cosmetic varicose veins".
 Venous leg ulcer due to varicose veins being diagnosed as "only cosmetic" and therefore not treated for 20 years
Venous leg ulcer due to varicose veins being diagnosed as "only cosmetic" and therefore not treated for 20 years
The result of this lack of action is evident in the picture. The patient went on to develop a venous leg ulcer. This appeared two years ago. District nurses have healed it on one occasion with compression bandages and dressings. However as no one treated the underlying varicose veins, the leg ulcer returned as soon as the compression was removed. The Whiteley Clinic has been campaigning now for over a decade and a half to try to get doctors, nurses and patients to understand that visible varicose veins are only a sign of underlying venous problem. This is usually venous reflux. Indeed Prof Mark Whiteley wrote a simple book in 2011 to help anyone understand this (Understanding venous reflux - the cause of varicose veins and venous leg ulcers).
Understanding venous reflux the cause of varicose veins and venous leg ulcers by Mark S Whiteley
Varicose veins are rarely cosmetic. The term "varicose vein" means a vein that is visible and bulging (i.e. varicose). About 15% of the population have visible varicose veins. Another 15% have venous reflux causing problems but not showing obvious varicose veins on the surface. We call these "hidden varicose veins". These patients often end up with leg ulcers, venous eczema and other complications of venous disease. There are few patients who really only have "cosmetic varicose veins". These are patients who have small thread veins or spider veins and no underlying hidden varicose veins. No doctor or nurse should ever diagnose "cosmetic varicose veins" unless they have had a venous duplex ultrasound scan performed by an expert clinical vascular scientist showing that all of the underlying veins are working normally. No patient should ever accept a diagnosis of "cosmetic varicose veins" or accept that they are not being referred for an expert opinion unless they have had a duplex scan to prove it. If this message was understood by doctors, nurses and patients, we would not have any patients like this poor gentleman who ended up with a venous leg ulcer because his general practitioner kept telling him he only had "cosmetic varicose veins". Fortunately for him, he found The Whiteley Clinic on the Internet and has now come for diagnosis and treatment. He will shortly be having endovenous laser treatment of his massive small saphenous vein, closure of his incompetent perforating veins with TRLOP and then eight weeks later, foam sclerotherapy. His leg ulcer will almost definitely be cured for ever 4 to 6 months after treatment and, as our research has shown, it is unlikely that he will ever need to wear compression stockings again. See our research on Leg Ulcers