Can Microsclerotherapy Effectively Remove Spider Veins?
July 18, 2026
Foam Sclerotherapy Research continues to offer crucial insights into enhancing varicose vein treatment safety and effectiveness. This article explains what foam sclerotherapy is, the types of veins it treats, how it works, possible discomfort, post-treatment care, and recent scientific findings including the foundational study published in July 2014 in the Journal of Vascular Surgery (Venous and Lymphatic Disorders) by researchers at The Whiteley Clinic. It also references a relevant video that further illustrates the procedure.
Foam sclerotherapy is a minimally-invasive outpatient procedure used for varicose veins and venous malformations or small varicosities. “Sclero” means hardening, and “therapy” means treatment. The procedure usually takes place in a clinic without surgery.
To begin the procedure, clinicians carefully inject a foam sclerosant into the affected vein, so that the damaged vessel can be treated directly.
The foam then breaks down the cells of the vein wall, deliberately injuring the inner lining so that the vessel collapses. Gradually, the body absorbs the treated vein, allowing blood to flow through healthier vessels.
As this process takes place, blood flows into healthier veins, which improves overall circulation.
Unlike liquid forms, foam has a thick consistency similar to shaving cream. Therefore, it effectively displaces blood and remains in contact with the vein wall for longer, which improves treatment success while simultaneously reducing risk. Furthermore, clinicians often apply the Whiteley-Patel modification, mixing the sclerosant with carbon dioxide and oxygen instead of air. This method improves safety and also helps the foam last longer.
clinicians can perform foam sclerotherapy under different conditions, temperatures, altitudes, and using various equipment. Essentially, the foam works on the damaged vein, closes it, and then channels blood toward the healthy venous system.
Foam Sclerotherapy Research shows the procedure is ideal for spider veins and smaller varicose veins that cannot be managed with compression stockings or weight control. Typically found on the legs, spider veins are delicate, web-shaped veins visible through the skin.
Veins up to 3 mm respond very well when clinicians apply foam correctly. However, effectiveness begins to decrease for veins between 4 and 5 mm, and consequently, larger veins often require alternative treatments, such as endovenous thermal ablation. Ultrasound-guided foam sclerotherapy ensures precise targeting, enhancing safety and results. Proper compression after treatment is crucial to prevent staining.
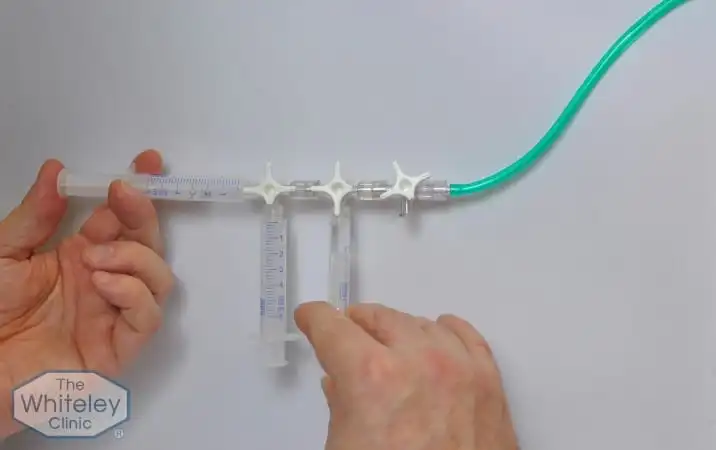
Foam sclerotherapy works through both mechanical and chemical actions. To begin with, clinicians create a foamed sclerosant using either a double-syringe or the modified three-syringe (Whiteley-Patel) technique. Subsequently, the foam pushes blood into healthy veins and intentionally disrupts the wall of the defective vessel. Eventually, the body naturally absorbs the damaged vein.
Furthermore, this approach proves particularly effective for tortuous veins and small varicose veins, thereby ensuring a higher success rate and better overall outcomes.
Patients generally experience minimal discomfort during foam sclerotherapy. Although the injection may sting briefly, wearing compression garments immediately afterwards for about 14 days helps prevent blood from re-entering the treated veins and reduces the risk of brown staining.
Foam Sclerotherapy Research shows that if the sclerosant foam is prepared using air, patients may experience visual disturbances, headaches, or migraines.
However, when clinicians prepare the foam using a mixture of carbon dioxide and oxygen, they can significantly reduce these risks. Additionally, patients may experience skin hyperpigmentation, although this usually improves over time or can be managed with minor interventions.
Patients should:
Following these steps helps patients recover more effectively, enjoy improved cosmetic results, and achieve long-term success. Moreover, Foam Sclerotherapy Research emphasises that strict adherence to compression and post-treatment care plays a crucial role in attaining optimal results.
Furthermore, to gain a clearer understanding of the patient experience and the procedural steps, you can watch the video whose transcript you provided. It demonstrates how foam sclerotherapy works, showing how the foam displaces blood, the importance of compression, minimal discomfort, and its suitability for veins up to 4–5 mm.
Foam Sclerotherapy Research highlights that not everyone is suitable for the procedure. Contraindications include:
Careful screening ensures safety and optimal results.
Foam Sclerotherapy works best when the foam effectively displaces blood and maintains prolonged contact with the vein wall. Therefore, Foam Sclerotherapy Research at The Whiteley Clinic examined how different external factors can influence foam longevity. For instance:
By understanding these factors, clinicians can create longer-lasting and safer foam, ultimately maximising treatment success while minimising risks.
Foam Sclerotherapy Research proves that optimised procedures, safer gas mixtures, and proper post-treatment care create a powerful, minimally invasive treatment for varicose veins. It treats small veins effectively, reduces discomfort, and provides strong long-term results. As new studies emerge, foam sclerotherapy remains a cornerstone of minimally invasive venous care.
For those who would like to explore the study in more depth, the clinical abstract of this Foam Sclerotherapy Research is available to read in full on The Whiteley Clinic’s published research page.