



Unveil the Hidden Causes of Varicose Veins for Permanent Treatment Results
February 19, 2026
PUBLISHED BY
Venous Perforator Surgery research published from The Whiteley Clinic proves that is reduces recurrences

From the The Whiteley Clinica; and the Faculty of Health and Biomedical Sciences, University of Surreyb, The Imaging Clinic, Mount Alvernia Hospitalc
Author conflict of interest: none.
Presented as a poster to a team of judges at the American Venous Forum, 26th Annual Meeting, New Orleans – February 2014.
Charing Cross International Symposium, London – April 2014. Oral presentation at this International conference
This study aims to challenge the longheld idea that the diameter of ovarian veins is of importance in the diagnosis of venous reflux. As can be seen on duplex ultrasound, veins of both large and small diameters display reflux, thus including a criterion involving vein diameter in diagnostic protocols is unnecessary. The article will hopefully prompt physicians to think twice about using diagnostic imaging techniques that place a heavy reliance on measuring the diameter of veins under investigation.
Previous research into pelvic venous reflux has suggested that the size of the ovarian veins indicates the presence or absence of reflux. It is already known that vessel diameter is not an indicator of reflux in the great saphenous vein. However, to this day, physicians still use vein size to plan treatment of refluxing ovarian veins. The authors aimed to investigate whether or not vessel diameter can be used as an indicator of reflux in the ovarian veins.
Nineteen female patients (mean 40.2 years, range 29–60) presenting to a specialist vein unit with leg varicose veins underwent duplex ultrasonography (DUS). All were found to have a significant pelvic contribution to their leg reflux on transvaginal duplex ultrasonography (TVS) and were referred to an interventional radiologist for treatment by transjugular coil embolization. During the procedure, the diameter of the ovarian veins was measured using digital subtraction venography.
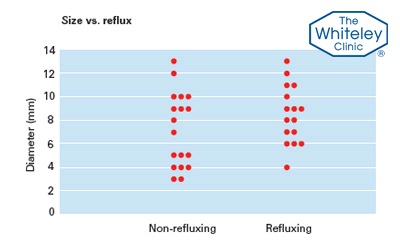
Thirty-four ovarian veins were measured (17 right, 17 left) and of these 18 were found to be nonrefluxing while 16 displayed reflux. The mean diameter of the non-refluxing veins was 7.2 mm (range 3–13 mm) and that of the refluxing veins was 8.5 mm (range 4–13 mm). This difference was found to be insignificant at a 95% confidence level (Student t test, p = .204).
There is no significant difference between the diameters of competent and refluxing ovarian veins and, as such, techniques that measure vein diameter may not be suitable for the diagnosis of venous reflux in the ovarian veins.
All female patients coming to The Whiteley Clinic with any of the symptoms or signs of pelvic vein reflux are offered a transvaginal duplex ultrasound (TVS) using the Holdstock-Harrison technique. As our vascular technologists invented the technique, everyone scanned is scanned by Judy Holdstock, Charlie Harrison or someone trained directly by them.
All female patients coming to The Whiteley Clinic with suspected pelvic vein reflux have the highest possible chance of an accurate diagnosis and therefore the best possible chance of getting the correct veins treated.
Scott J. Dos Santos (The Whiteley Clinic Summer Research Fellow 2013 and The Whiteley Clinic Summer Research Co-ordinator 2014, 2015 & BioMed Student)
Judith ‘Judy’ M Holdstock (Chief Vascular Technologist, The Whiteley Clinic)
Charmaine ‘Charlie’ C Harrison (Senior Vascular Technologist, The Whiteley Clinic)
Anthony J. Lopez (Consultant Radiologist)
European Journal of Vascular and Endovascular Surgery. 2014 Nov 22. pii: S1078-5884(14)00582-6. doi: 10.1016/j. ejvs.2014.10.013. [Epub ahead of print]
American Venous Forum, 26th Annual Meeting, New Orleans – February 2014. Presented as a poster to a team of judges Charing Cross International Symposium, London – April 2014 Oral presentation at this International conference.
This graph shows that the size of the ovarian vein does not indicate whether it is normal or whether it is refluxing blood. This shows that transvaginal duplex is the gold standard test for pelvic vein incompetence. Venogram, MRI or CT depend on measuring the diameter of the vein and so are less accurate. Research published from the The Whiteley Clinic.
Most doctors use MRI, CT scanning or Venography to try to diagnose pelvic vein reflux. These techniques usually have the patient lying flat (not good for looking for varicose veins and venous reflux!) and so they use the size of the vein to judge if the vein is working or not.
Why would they be looking for pelvic vein reflux? Well pelvic vein reflux is what causes:
Since the year 2000, The Whiteley Clinic has been spearheading the research into pelvic vein reflux and how both diagnose and treat it.
Our vascular technologists – Judy Holdstock and Charlie Harrison – developed the technique of using Transvaginal Duplex Scanning (TVS) to diagnose pelvic vein reflux. This technique is now widely known as the ‘Holdstock-Harrison Technique’. Duplex is the gold standard test for blood flow in veins and is fantastic to see venous reflux.
The study compared the size of the vein measured at coil embolization, using the catheter as a measuring stick. We were then able to compare the sizes of normal veins with no reflux against those with pelvic vein reflux.
As we suspected, there was no correlation at all between the size of the vein and whether it was working or not. We found normally functioning ovarian veins came in all sizes – and also abnormally refluxing ovarian veins came in the same wide range of sizes.
This research is of huge importance as most radiologists still report that ‘small veins’ are ‘normal’ and ‘large veins’ are ‘abnormal’. What is worse, they then recommend treatment on these findings of size from MRI, CT scanning and venography.
Hence doctors who treat patients with pelvic vein reflux and who don’t use the Holdstock-Harrison technique for transvaginal duplex ultrasound scanning – but instead rely on size estimations by MRI, CT scanning or venography – are likely to be treating a lot of normal but large veins, and missing a lot of small but abnormal veins.
This shows that every woman having treatment for pelvic vein reflux – or indeed being told they don’t need treatment – must have a TVS performed using this technique.
Reference: https://www.ncbi.nlm.nih.gov/pubmed/25457295
The reason this study was performed was the increasing numbers of patients coming to The Whiteley Clinic having had Pelvic Vein Embolisation performed elsewhere – only to find that their problems did not change after the procedure.
All had been diagnosed and treated on the basis of MRI, CT Scanning or Venography.
Transvaginal duplex ultrasound scanning then performed by the specialist team at The Whiteley Clinic found that in each case, the wrong veins had been treated or the embolization procedure had been performed inadequately.
We believe that this shows that no patient should have a diagnosis of pelvic vein reflux either made or refuted without having had a TVS using this technique.

