Deep Vein Thrombosis
What is Deep Vein Thrombosis?
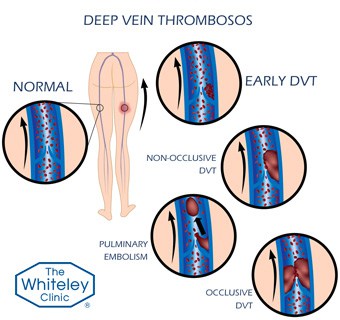 A deep vein thrombosis (DVT) is an abnormal clot that has formed in the deep veins of the leg or pelvis. They have become feared by the general public for very good reasons. In the short term, large DVTs can move from the leg or pelvic veins and go through the venous system travelling into the heart and then lungs. This is called a pulmonary embolism (PE) which is a very serious medical condition and can even be fatal. In the long term, even when DVT’s have been successfully treated, the scar tissue formed in the deep veins can lead to a problem called post thrombotic syndrome (PTS). This PTS can result in discoloured, uncomfortable and swollen legs which may even end in leg ulcers.
A deep vein thrombosis (DVT) is an abnormal clot that has formed in the deep veins of the leg or pelvis. They have become feared by the general public for very good reasons. In the short term, large DVTs can move from the leg or pelvic veins and go through the venous system travelling into the heart and then lungs. This is called a pulmonary embolism (PE) which is a very serious medical condition and can even be fatal. In the long term, even when DVT’s have been successfully treated, the scar tissue formed in the deep veins can lead to a problem called post thrombotic syndrome (PTS). This PTS can result in discoloured, uncomfortable and swollen legs which may even end in leg ulcers.
Although most DVTs are small, harmless and resolve by themselves, it is also true that a great many DVTs never get diagnosed and are often passed of by patients, doctors and nurses as “muscle sprains” or other leg aches. Without a venous duplex ultrasound scan performed by a specialist vascular scientist (who is able to scan even the smallest veins in the calf), one cannot be certain as to whether a DVT is present or not.
As such, it has become essential to diagnose DVTs using the very best duplex ultrasound machines by experienced vascular scientists. These specialists are able to perform very detailed and accurate scans to ensure that any DVT is identified and treated accurately. Screening blood tests and quick duplex scans performed in a matter of minutes can exclude some major DVTs and regularly miss DVTs that might cause significant problems if left.
A Duplex ultrasound scan should also be used to identify when the DVT has fully resolved enabling a recommendation as to when Warfarin or other anticoagulation can be stopped safely. Traditionally doctors have given a standard course of Warfarin, usually 3 or 6 months, and then stop anticoagulation without checking whether the DVT has actually resolved or identify if it is has caused any damage to the deep veins. As part of The Whiteley Protocol®, we not only use duplex ultrasound scanning to accurately diagnose DVT but also to check that any treatment has been successful to ensure that each treatment regime is tailored to each individual patient.
Finally, it is essential to find out whether there is a cause for a DVT. In many cases there is an obvious cause – such as surgery, dehydration or a long flight whilst on the oral contraceptive pill. However, recent interest has focused upon patients who get a DVT for no known reason – a so-called ‘unprovoked’ DVT. Such patients need to be checked to make sure they do not have a hidden cancer as this can be a major cause of an unprovoked DVT.
Understanding Blood Flow & Deep Vein Thrombosis
Blood Flow in Arteries
Arteries are the blood vessels taking blood away from the heart. The heart is a very powerful muscle – so the blood is ejected out at a high velocity and with high pressure. As the heart beats approximately once every second, the pressure and flow increases once per second. To withstand this regular increase of flow and pressure, the arterial walls have to be strong (to withstand the pressure), elastic and muscular (to dilate when the pressure pushes outwards, and to bounce back to normal shape when the pressure pulse passes.
The walls of the arteries have 3 main layers and a special lining that is contact with the blood. It is the Media that gives the arteries the ‘bounce’ and lets them return to their normal shape after the heart has pumped blood through them at high pressure. You can feel this ‘bounce’ in some areas of the body such as at the wrist – this is called the ‘Pulse’.
Blood Flow in Veins
Veins are the blood vessels that carry blood back to the heart from the tissues. These tissues might be in the legs, arms, brain, liver, lungs etc.
Of course, it can easily be seen how blood returns from the brain – provided you are standing or sitting upright, gravity will do the work for you. However, to get blood back to the heart from below it, the blood needs to be “pumped up” against gravity.
It is the understanding of the venous pump in the legs – and more importantly its failure – which leads to the problems of varicose veins, venous eczema, lipodermatosclerosis and venous ulceration. However, as far as an understanding of the veins is concerned in relation to deep vein thrombosis, we can concentrate on the flow in a patient at rest, who is lying down and whose flow is steady and not being pumped.
The vein wall has the same layers as the arterial wall, but it is much thinner. It is thinner as the flow is smoother and the vein wall does not have to withstand the pressure of the heart pumping.
The endothelium, intima and adventitia layers are much the same – the difference in the wall thickness is due to the the Media layer (the muscle layer) being much thinner.
Blood flows back to the chest from the legs through the veins.
As we have said, the blood is not being pushed back by the heart and so it has Low Pressure and fairly smooth Flow when you are lying down at rest. It is for these 2 reasons that veins do not Pulsate – which is why you can’t feel a pulse in the veins – only in the arteries.
Therefore,the important things to realise at this stage are:
- Veins contain blood flowing smoothly and at low pressure
- Veins have thin walls but still have endothelium next to the blood which stops the blood from clotting inside the vein.
Blood Flow in Leg Veins when sitting & standing
Things change in the veins when we sit or stand up. This is particularly important when we consider sitting in an airplane. When a DVT occurs in this situation, it is called ‘Economy Class Syndrome’ or ‘Traveller’s Thrombosis’.
However, you should be aware that research suggests that there is a difference between air travel and coach travel. It appears there is a higher risk of DVT on a flight than during the same time sitting in a coach. This is probably due to the oxygen being ‘thinner’ during a flight (most commercial aircraft are pressurised to 7,000 – 12,000 ft – so there is less oxygen in each breath than at ground level). This is obviously not the case in a coach.
Nevertheless, as we try to stop DVT and ‘Economy Class Syndrome’ or ‘Traveler’s Thrombosis’ by encouraging movement, compression socks (travel socks) and hydration, it is useful to understand the changes that occur when sitting.
Most people do not get swelling of the ankles when they sit still for long periods of time. The way they get around this problem is by using their ankles to pump blood back to the heart. By continually moving every few minutes or so, they use the muscles of the legs to pump the blood back up to the heart.
As the vein system is a Low Pressure system, whenever the heart is above the ankles, blood cannot flow smoothly back. In fact, it cannot flow up the veins at all by itself as there is nothing pushing it upwards against gravity.
Instead it collects at the ankles and, if we sit still enough for long enough, the ankles will swell. This is due to the increasing pressure in the blood at the ankles as it starts collecting here, pushing outwards against the vein walls. Eventually the pressure reaches a sufficient level that fluid is squeezed out of the blood, through the vein walls and into the tissues. This swelling due to fluid is called oedema.
Symptoms of DVT
The possible symptoms of Deep Vein Thrombosis can include:
- Tender leg for no obvious reason – can be above knee, below knee or both
- Swelling of ankle, ankle and calf, ankle, calf and thigh or even the whole leg
- A heavy ache in the leg – especially on standing or walking
- Warm skin in area of swelling
- Sometimes the skin can be a bit redder but this is more common in phlebitis (inflammation of the vein wall)
- DVT usually affects one leg, however it can affect both.
DVT usually affects one leg, however it can affect both.
Sometimes (estimated to be 50% of pateints) there are no symptoms and a DVT is only diagnosed if a complication occurs.
Causes of Deep Vein Thrombosis (DVT)
Blood is fluid when it flows through the arteries and veins. However it has to be able to clot in certain circumstances – for example to stop bleeding after a cut or graze.
In some circumstances the blood can clot when it still inside a blood vessel. When blood does this, either within an artery or vein, it is called a Thrombosis. The actual clot itself is called a thrombus – the condition of having a thrombus in a blood vessel is called thrombosis.
If a thrombus breaks away from the blood vessel wall and moves through the circulation with the blood, it is called an embolus. The condition caused by an embolus moving and getting stuck somewhere – often in the lungs – is called embolism.
A famous pathologist called Virchow pointed out in the 1920’s that there are 3 main causes for blood to clot when it is still in a blood vessel. These three factors are called – Virchow’s Triad.
- Changes in the blood vessel wall
- Changes in the blood flow
- Changes in the blood composition
Changes in the blood vessel wall
Blood vessels are lined by a special sort of cell called an endothelial cell. This is a very flat sort of cell that has special properties, preventing normal blood clotting on it. Anything that damages the endothelial cell, can cause blood to clot on to it or to clot to the lining of the blood vessel underneath the endothelial cell.
Things that damage the endothelial cell include smoking or low oxygen concentrations.
The vessel wall can also change by having scars on it – such as having previous deep vein thrombosis – or bulges and narrowings of the vein walls as in varicose veins.
Changes in the blood flow
Humans, like all animals, really needs to be quite active. Unfortunately with modern day life, there are many instances where we are less active than we should be.
These might be for reasons we are unable to avoid, such as illness or breaking a leg, but also often due to our way of life such as sitting for long periods in front of a computer or television, travelling in cars, coaches or aeroplanes. By reducing the activity of the leg, the muscle pump is infused and so the blood flow becomes very sluggish in the deep veins.
Another cause for a change in the blood flow would be a change in the diameter or length of a vessel – such as found in varicose veins. Instead of the blood flowing smoothly up a narrow straight vessel, varicose veins with their bulges, narrowings, curves and kinks means the blood flow is altered and so clots are more likely to form.
Changes in the blood composition
The commonest cause of blood composition changes is dehydration. This often occurs because people drink alcohol or drinks with caffeine in them such as tea, coffee or some soft drinks. Unfortunately alcohol and caffeine act as diuretics, meaning that although fluid is being taken in, more is passed out in the form of urine. Therefore the blood becomes more concentrated and more likely to clot.
Females taking oestrogen either in the form of the oral contraceptive pill or as HRT, are also changing the blood composition in a way that makes thrombosis more likely. People with high blood fats (hyperlipidaemia) are also more likely to get clots due to an abnormal blood composition.
Deep vein thrombosis and cancer
Over the last few years, it has become increasingly well understood that deep vein thrombosis (DVT) can be the first sign of an underlying cancer, particularly in people over 40 years old.
The reason for this is not fully understood but it is likely that certain cancers, particularly of the bowel, breast, lung or pancreas secrete certain substances into the blood that increase the risk of DVT.
As such, anyone who is found to have a DVT for no good reason (a so-called ‘unprovoked’ DVT) should undergo full physical examination and tests to look for these common cancers.
‘Standard’ prevention, diagnosis and treatment of DVT
Most people who are doing things at high risk of Deep Vein Thrombosis DVT are given advice or help to reduce the risks:
- When flying you are advised to wear properly fitted flight socks and to keep well hydrated
- When having a general anaesthetic most patients have either TED stockings or heparin injections – or both
- When in the heat, you are advised to drink water to keep well hydrated
Tests & Scans for Deep Vein Thrombosis
The Whiteley Clinic only use gold standard testing to diagnose DVT – a duplex ultrasound scan performed on a high resolution machine by our own trained vascular scientists working to The Whiteley Protocol®. All of our vascular scientists scan veins regularly and are experts in all aspects of venous scanning. To make sure no DVT goes unmissed, all veins are checked from groin to ankle and often even into the pelvis. We would never use the quick alternative that is often used by doctors or clinics as a quick screening test which only takes a few minutes and is quite likely to miss significant DVT.
We do not specify how long treatment should last. Instead, we use venous duplex ultrasound scanning to tailor the treatment that each patient needs, which is dependent on how well they are responding to anticoagulation. By doing this, we have often avoided stopping Warfarin too soon (when clot is still present), or avoided stopping it in patients who have narrowed veins who should stay on the Warfarin to prevent further DVTs.
Testing for DVT
When DVT is suspected, a variety of tests are used to screen for it:
- Venography – An X-ray with contrast injected into the foot – now out of date and not needed
- Thermography – an infra-red device is used to see if the leg is warmer than the other – quite inaccurate and useless if both legs have DVTs!!
- Blood test – tests checking for signs of clots in the blood are simple to perform, and although often right do sometimes give the wrong results. This means either patients get treatment they don’t need until a specialist scan is done, or get sent home with a DVT
- Duplex Ultrasound scan – this is the gold standard – but only if done by a specialist who checks from pelvis to ankle (taking 30 mins +). Many non-specialists or doctors or nurses who have “been on a course” will be able to see a massive DVT in the thigh, but will often miss small DVTs in the lower leg, where the veins are tiny.
- Treatment is usually with Heparin injections then oral Warfarin tablets. The level of anti-coagulation (clotting level) is regularly checked with the INR blood test. Warfarin is usually stopped 3 or 6 months after the diagnosis of the DVT.
- A painful swollen leg is the commonest presentation of a deep vein thrombosis (DVT). However many other things cause painful swollen legs and also some DVTs present without pain, or without swelling. Therefore, before we think about treatment of DVT, we have to make sure that we are treating a deep vein thrombosis and nothing else instead.
Blood tests for DVT
There are some blood tests that are used in accident and emergency departments for screening for deep vein thrombosis (DVT). These rely on picking up the biochemical markers of clotting somewhere inside the circulatory system.
An argument can (and has) been made for these tests as a screening test to put people into a high risk” or “low risk” category of having a DVT. this is useful in a public service that has a lot of people to see and where costs have to be contained. However, these are not highly accurate and so in an individual who wants tohave the optimal treatment, there is really no place for them.
Duplex Ultrasound scan
The best test currently available for diagnosing deep vein thrombosis (DVT) is a colour flow duplex ultrasound performed by a specialist. There are several different sorts of colour flow duplex ultrasound and to be able to diagnose small deep vein thromboses in the calf, a very high resolution machine is required operated by someone who is expert in scanning veins.
At The Whiteley Clinic we insist on the very best equipment and train our own vascular scientists to make sure that they reach the exacting standards that we insist upon.
DVT Treatment & Therapy
The usual treatment for deep vein thrombosis is to thin the blood using anticoagulants.
This usually entails injections of heparin which act immediately, whilst oral warfarin is started and stabilised. Warfarin combats the vitamin K in the body which is used for blood clotting. It is usually started by giving a loading dose for three days and then using blood tests to stabilise the right dose over the next few days to weeks.
The correct level is obtained by measuring the clotting time by a regular blood test – the “INR” (International Normalised Ratio). For DVT this should be kept about 2.0 – 3.5 x normal clotting – in other words, the time for the blood to clot should be 2.0 – 3.5 times longer than it would normally clot in that person.
The body is able to break down most clots by itself and so the heparin followed by the warfarin is merely there to stop any more clots forming whilst the body breaks down the deep vein thrombosis (DVT) that is already there.
Traditionally doctors have kept the warfarin going for three to six months. However, we now rescan the leg to make sure the blood is flowing before deciding whether the warfarin can be stopped or not.
Very rarely, if there is a massive deep vein thrombosis which is a risk of either blocking the veins completely or breaking off and going up through the system to the lungs (a pulmonary embolism), then either a clot busting injection called thrombolysis can be used to break down the clot, or a filter can be put into the veins to catch the clot if it breaks off.
Superficial Thrombophlebitis (Phlebitis)
Clots in the superficial veins are painful and locally inflamed and lumpy. Once the diagnosis has been confirmed, treatment is usually non-steriodal anti-inflammatory drugs such as Aspirin in those who can tolerate them.
Antibiotics are NOT needed as the inflammation is due to the clot in the vein and NOT infection.
In severe cases, the clot can be removed under local anaesthetic, reducing the pain, speeding up the recovery and improving the end cosmetic result.
In the longer term, the underlying cause needs to be treated – usually varicose veins.
Post-Phlebitic Limb
Treatment of the post-phlebitic limb can be a very complex and demanding process – often requiring considerable time and expense.
Fortunately, most people who consult us having been told elsewhere that they have “complex veins” or a “post-phlebitic limb” actually turn out to have less severe and more easily treatable conditions once we have performed our specialised scans.
Those rare people who do have complex post-phlebitic limb are given a full diagnosis and explanation, and a full option of possible treatments are discussed. As these are many and varied, they cannot be easily summarised here.