Leg Ulcers
What are Leg Ulcers and how are they treated?
Leg ulcers are open, non-healing wounds of the legs. They are usually on the lower legs or the feet. They can be thought of as “open sores”.
Ulcers can be painful or not painful. They can be big or small, wet or dry, smelly or not smelly. Leg ulcers can have many different appearances. Therefore, it can be very confusing if they are only assessed by their appearance. Many nurses and dermatologists use the surface appearance as part of their assessment – often leading to incorrect diagnosis and sub-optimal care (see below).
There is little information that can be gleaned just by looking at the ulcer. However, a rare skin cancer called a Marjolin’s ulcer can be noted by seeing a “rolled edge”. So although not the most important part of the assessment nowadays, it is still essential to have a look at the ulcer itself.
As stated above, there is very little that can be found just from looking at a leg ulcer in the majority of cases. Unquestionably, it is impossible to tell if a leg ulcer is curable or incurable just from looking at the surface alone.
Definition of “Leg Ulcer”
The word ‘ulcer’ means a break in the layer of cells forming a surface. This is called the “epithelial layer” and epithelial cells line any outside surface of the body.
Hence ulcers can occur in many different areas of the body. Ulcers cause different problems depending on what surface they are breaking up. For example, a stomach ulcer is a break in the cells forming the lining of the stomach. This allows gastric acid to attack the underlying tissue. This can result in pain, bleeding or even perforation. A more common ulcer is a mouth ulcer. Most of us will have had one at some time. This is a break in the mucosal cells lining the inner surface of the cheeks. It allows saliva to get the underlying tissue and causes severe pain.

In the case of leg ulcers, the skin breaks down and this allows air and bacteria to get into the tissue below. When an ulcer occurs on the leg, it is tempting to cover it up, hoping the skin will grow back. This is why humans, throughout history, have put dressings over leg ulcers, hiding them away and hoping they will heal.
However, such simple actions miss out one major point. By covering the ulcer, the person doing the covering is not thinking about why the ulcer occurred in the first place.
Underlying causes of Leg Ulcers:
Since the 1990’s, research has shown that the real root cause of a leg ulcer appearing is abnormal blood supply to the skin. Occasionally it is blood supply taking nutrients to the skin. However, in most cases, this is due to varicose veins or “hidden varicose veins”. In these cases, the veins are failing to take the venous blood away from the leg. This causes inflammation and skin damage,
That is why we follow The Whiteley Protocol® In the protocol, we find the underlying cause of the leg ulcer using high-resolution duplex ultrasound. This is done by a The Whiteley Clinic trained vascular technologist. Once the underlying cause has been found, the protocol then points out the best route to curing the problem and hence the leg ulcer.
We have now proven this at The Whiteley Clinic showing that we cure 85% of venous leg ulcers using The Whiteley Protocol. This is a permanent cure (not just “healing” with dressings), and 52% of patients never need compression again.
Types of venous leg ulcers:
There are 3 main causes of leg ulcers:
- Venous
- Arterial
- Other Causes
Venous leg ulcers:
are caused by veins not working properly – about 80-90% of leg ulcers. Most of these are due to the valves not working – varicose veins or “hidden varicose veins”. Often this also includes incompetent perforating veins although many surgeons do not treat these. At The Whiteley Clinic we invented the TRLOP technique (see below) and so all of our doctors treat incompetent perforating veins. Venous leg ulcers are treated by venous surgeons or phlebologists. Vascular (arterial) surgeons often fail to treat perforating veins or other more subtle causes of venous leg ulcers.
Other venous causes include obstruction where the vein is narrowed or blocked, or stasis. Fortunately, these are uncommon.
Arterial leg ulcers:
are caused by the arteries not working – about 5-10% of leg ulcers. Arteries take blood and nutrients to tissues. When they become narrowed or blocked, the skin doesn’t get nutrition. Although uncommon, arterial ulcers are easier to understand and to treat. They are treated by vascular (arterial) surgeons.
Other leg ulcers:
are caused by rarer conditions – about 5% of leg ulcers. Such ulcers can be caused by infection, auto-immune diseases or connective tissue conditions, amongst other causes.
Please note that specialists like the venous surgeons at The Whiteley Clinic, always check for other causes, such as arterial causes, before treating venous leg ulcers. This is essential as many leg ulcers occur in older people and they may have more than one cause for their leg ulcers.
The ‘Old Understanding’ of venous Leg Ulcers
Until the 1980s, most doctors and nurses had a clear understanding of the difference between venous leg ulcers and varicose veins.
Unfortunately, it turned out that they were wrong!
When valves failed in the superficial veins, they swelled on the surface causing varicose veins.
They believed that the deep veins could not be treated and so the only way to treat venous leg ulcers was to wrap the leg in compression bandages and dressings.
They also believed that the superficial veins caused no inflammation. Although they could be treated by varicose vein surgery, there was no need to do so as varicose veins were “only cosmetic”.
They believed in only 2 systems of veins in the legs – the deep and superficial systems. The deep veins were in the muscles. The superficial veins in the fat under the skin.
When valves failed in the deep veins, this resulted in inflammation at the ankles. After a time, this inflammation would accumulate until the ankles swelled, the skin turned brown and leg ulcers appeared.
It is a great pity that many doctors and nurses still believe this, as it is totally incorrect.
This error has resulted in patients with leg ulcers failing to get the right treatment and ending up in compression for years. It also resulted in patients with varicose veins being left untreated, deteriorating towards complications such as leg ulcers in the future.
The ‘New Understanding’ of Leg Ulcers
In the late 1980’s, a new test called Duplex Ultrasound was invented.
Duplex ultrasound allowed us to see the veins, and also see the blood flowing within them. Researchers using duplex ultrasound quickly found that the previous understanding of venous leg ulcers and varicose veins was completely wrong.
Research published in the 1990s showed that most venous leg ulcers were caused by superficial vein reflux. Previously, it had been thought that when the valves failed in the superficial veins, the superficial venous reflux that resulted only casued varicose veins. The valves failing allow blood to fall the wrong way down the veins – a process called “reflux”. This reflux was thought to stretch the wall of the veins, causing varicosities.
However, this new research found that the majority of venous leg ulcers were caused by superficial vein reflux. Deep vein reflux alone was found in only a minority of cases.
Even more interesting, many of the patients with superficial vein reflux did not even show varicose veins on the surface. This gives the term “hidden varicose veins”.
The results of this research are startling. It means that:
- Most venous leg ulcers are curable by varicose vein surgery
- No one can tell the cause of a leg ulcer without a venous duplex ultrasound scan
- Varicose veins are not cosmetic as they can go on to cause venous leg ulcers
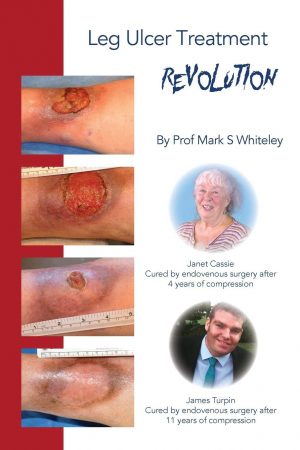
Leg Ulcer Treatment Revolution – by Prof Mark S Whiteley
Further developments in Curing Venous Leg Ulcers:
Developments since have been equally valuable. There is still no easy way of treating deep valve failure. Conversely, we treat superficial valve failure with ablation. Introduced into the UK in 1999 by Mark Whiteley, the ablation of superficial venous reflux is highly successful even in the long term. We have now shown our 15 year success rates in a study published from The Whiteley Clinic.
This is excellent news for our patients at The Whiteley Clinic.
Provided the patient can walk, most are now curable.
Research has continued. Deep vein reflux is usually secondary to a deep vein obstruction at a higher level. Placing an expandable metal tube called a “Stent” through such obstructions, opens them up and holds them open. Therefore in many cases, even deep vein problems are now curable.
As such, no patient who can walk should ever accept long-term dressings and compression for a leg ulcer unless they have been fully investigated by an expert team.
If you want to know more about venous leg ulcers and how they can be cured permanently, see “Leg Ulcer Treatment Revolution” published in November 2018. This is available on Amazon and in good bookshops.
https://www.amazon.co.uk/Ulcer-Treatment-Revolution-Mark-Whiteley/dp/1908586052/
Causes and Symptoms of Leg Ulcers
A better understanding of the causes of Leg Ulcers has helped establish Leg Ulcer treatment, which can permanently cure a long term problem.
The two major causes of all Leg Ulcers are venous (veins not working, which accounts for about 80% of Leg Ulcers) and arterial (arteries not working, which accounts for about 15% of Leg Ulcers). However, there are rarer causes and considerations for diabetic and malignant Leg Ulcers, which are also outlined below.
We will focus on venous Leg Ulcers as they are the most common and, with specialist treatment, often the easiest to cure. A good vascular surgeon will nonetheless check for arterial and other causes before commencing treatment. Patients may have more than one cause of Leg Ulcers, and even though a venous origin may be found, there could also be arterial or other issues present at the same time.
Fortunately, most arterial Leg Ulcers can be cured by bypass surgery or angioplasty. So by accurately identifying the cause (or causes), the appropriate treatment protocol can be formulated, often utilizing a combined approach of treating the arterial issues first, followed by the venous cause.
The remaining 5% of diabetic and malignant Leg Ulcers may equally be open to treatment.
Symptoms of Venous Leg Ulcers
Most Leg Ulcers are venous in origin and can be caused by:
- varicose veins
- hidden varicose veins
- venous reflux
- deep vein problems such as old thrombosis and scarring
- deep venous reflux, narrowings or blockages
As there are a number of different underlying venous causes for Leg Ulcers, so there can also be a wide variety of symptoms.
Leg Ulcers can, at times, be painful. This is often due to infection on top of the Leg Ulcer, or to the physical irritation and chafing of dressings, bandaging or compression bindings.
The severity of venous disease of the legs which is severe enough to cause Leg Ulcers can also cause swelling of the lower legs. This swelling can itself cause symptoms, with the skin feeling tight and the leg feeling heavy or full. Often there is itching of the skin, or tension in the skin due to the inflammation and swelling.
However, venous Leg Ulcers can also sometimes be asymptomatic, causing no pain or discomfort, although there will still be an open break in the skin requiring dressings.
Classically, venous Leg Ulcers improve and any associated pain reduces when the patient is lying down and the leg is elevated, as gravity works with the body to drain the venous blood out of the leg. Conversely, as the leg is below the level of the heart, when the patient is sitting or standing, the venous Leg Ulcers worsen.
Symptoms of Arterial Leg Ulcers
Arterial Leg Ulcers occur when there is not enough pressure in the arterial blood to force it through the capillaries in the toes, feet or lower ankles. If arterial blood does not go through these capillaries, then the vital supplies of oxygen and food such as glucose do not get to the tissues.
In addition, waste products from the tissues, such as carbon dioxide, urea and water, are not removed and therefore remain in the tissues. The combination of lack of oxygen and food and the accumulation of waste products damages the tissues and causes many cells to die. This tissue damage is almost always painful, making that a key symptom of arterial Leg Ulcers.
Contrary to the case with venous Leg Ulcers, the pain from arterial Leg Ulcers is usually improved when the legs are below the heart, particularly when the patient is sitting or standing. This is because gravity helps the flow of blood from the heart to get to the capillaries in the ankle, feet and toes. Conversely, the pain of arterial Leg Ulcers is made worse when the leg is elevated, for instance when the patient is lying down, as gravity is working against the flow of blood to the tissues in the lower leg, or foot and is worsening the condition. Consequently, many people with arterial Leg Ulcers often get out of bed at night, hang their leg out of the bed, or walk around, perhaps to sit in a chair.
Symptoms of Diabetic Leg Ulcers
Although many doctors and nurses refer to ‘diabetic Leg Ulcers’, these are almost always arterial Leg Ulcers that just happen to be occurring in a patient with diabetes.
In diabetes, the small capillaries may be damaged as well as the major blood vessels (arteries), so ulceration is more common and often more severe. Even more importantly, one of the problems with diabetes can be a loss of sensation in the toes, feet and lower legs. When this happens, what would ordinarily be a very painful arterial Leg Ulcer becomes asymptomatic and diabetic patients may not even realise that they have this additional condition. As a result, they often do not seek medical care or treatment until the ulcer has become severe, or grossly infected.
For this reason, The Whiteley Clinic strongly recommends that anyone with diabetes and any breakdown of the skin should consult a specialist doctor or nurse as soon as possible.
Symptoms of Malignant Leg Ulcers
One other rare but important type is the malignant Leg Ulcer. Quite often, this is actually a venous Leg Ulcer that has not been cured and has simply left open for a great many years. They are often referred to as a “Marjolin’s Ulcer”.
A Marjolin’s Leg Ulcer usually shares the same symptoms as any other underlying venous Leg Ulcer, and can therefore often be ‘asymptomatic’, hence the reason patients either do not seek advice, or why they might only have only been offered the traditional dressings and not a cure. The fact the Leg Ulcer has not been treated for so long is probably the reason it has become malignant.
In all the above cases, an appointment at The Whiteley Clinic is the first step in achieving a long-term cure for Leg Ulcers and swapping the pain of the condition and the inconvenience of traditional NHS dressings and bindings for pain-free, ulcer-free quality of life!
Diagnosis and Prevention of Leg Ulcers
How do we identify them? How early can we identify them? And what can we do to help prevent them occurring in the first place?
Although a fully-formed Leg Ulcer is an obvious condition to diagnose and identify, it’s often far more difficult for doctors and nurses to spot the key signs of patients who are still at the early stages of heading towards ulceration. It’s all too easy to miss a golden opportunity to prevent the worst symptoms ever actually developing.
It’s always advisable to seek specialist opinion and, increasingly, people with severe varicose veins are quite correctly bypassing NHS doctors who give the old advice of “…leave them until they cause a problem”. However, there are also many people with superficial vein valve failure who present with inflammation of the skin, but because the veins have not dilated, no varicose veins can yet be seen. These people are equally at risk of ulceration and we welcome seeing them at The Whiteley Clinic, precisely because it gives us the chance to prevent further serious problems with Leg Ulcers before they occur.
Early warning signs
One of the early warning signs is a pink, red or brown patch of skin (or the appearance of shiny, hard skin) on the lower leg, just above the ankle, usually on the inner side. This is called Lipodermatosclerosis (LDS). Without treatment – or if creams or pressure stockings are incorrectly prescribed, instead of making a referral to a specialist Vascular Surgeon – this slowly deteriorates to form a dark brown staining called Haemosiderin. If left untreated for longer, white patches then appear in the skin, indicating that the skin itself is breaking down. This condition rapidly leads to ulceration.
In fact, at any stage in this process, a referral to a specialist vascular surgeon would have been likely to result in definitive treatment that would not only stop further deterioration but often manages to reverse the process.
One note of caution – if the patient is not able to trigger their own internal, natural ‘leg pumping action’ – either through an inability to walk or due to poor ankle movement – then, unfortunately, surgery is unlikely to help. There is little to be achieved by stopping the reflux that happens after blood has been pumped if no pumping effect has been generated in the first place.
So to recap, the people most likely to benefit from a Leg Ulcer assessment at The Whiteley Clinic are:
- patients with a Leg Ulcer who are able to walk and who have reasonable movement of the ankle joint
- patients with pink, red or brown skin discoloration, or shiny hard skin, on the lower leg, usually just above the ankle
- patients already suffering from severe varicose veins and therefore at greater risk of Leg Ulcers
Venous Leg Ulcer Treatment
We specialise in liberating leg ulcer sufferers from the misery of bandages, dressings and uncomfortable bindings!
The National Institute of Health and Clinical Excellence (NICE) issued clear clinical guidelines in July 2013 that anyone with symptomatic varicose veins, a healed Leg Ulcer or an active Leg Ulcer should be referred for treatment at a specialist vascular clinic.
Traditionally, under NHS treatment, many people with Leg Ulcers have suffered needlessly from being condemned to the chore and discomfort of constant dressings and compression leg bindings. However, at The Whiteley Clinic, these outdated methods have been replaced by the most effective, most up-to-date and least surgically invasive procedures, often performed under local anaesthetic. And in a recent paper published in the peer-reviewed international medical journal ‘Phlebology’, it was demonstrated that The Whiteley Clinic has achieved an 85% cure rate for patients presenting with Leg Ulcers over the last 12 years.

This does not mean that our Leg Ulcer treatment follows a set pattern. Every patient is unique and before decisions are made, each person will be assessed by one of The Whiteley Clinic specialists. There may be cases where a cure is not possible; but for all patients, the best path to successful treatment is early investigation and diagnosis of the underlying conditions by our specialist ultrasound technicians using the best equipment available.
At The Whiteley Clinic, our own specialist ultrasound technicians follow The Whiteley Protocol®, an internationally recognised system for investigation and optimal treatment, and it is widely acknowledged that they are usually more experienced than consultants in this field, often going on to achieve full cures in people who have been told their Leg Ulcers are incurable.
The Procedure
Following an assessment by a The Whiteley Clinic trained Doctor specialising in Leg Ulcer treatment, patients will then be referred to a series of recommended tests. This will often be in the form of Duplex Ultrasound of veins and arteries, which may be accompanied by a Photoplethysmography scan (PPG), perhaps followed by further tests such as intravascular ultrasound (IVUS), venography, CT or MRI scanning.
The specialist will then discuss the results in depth, along with the best treatment options, with relatives or friends who will be involved in post-operative care invited to sit in on the discussion.
Endovenous Laser Ablation (EVLA) – a method of treating the underlying cause of Leg Ulcers using laser under local anaesthetic – is suitable for many patients.

Non-surgical options can accompany EVLA treatment, including manual lymphatic drainage.
The Whiteley Clinic does NOT recommend:
- Patients with leg ulcers should not be condemned to dressings and compression bandages without assessment by a specialist, or without a Venous Duplex Ultrasound scan performed by a skilled scientist. They can carry out an extended scan of all the veins of the leg, often in about 30 minutes.
- Patients with skin changes at the ankle should NOT be given creams (particularly steroid creams) before venous causes have been excluded. As noted above, an in-depth scan and an assessment by a specialist doctor should always be performed as an initial step.
- Patients with skin changes at the ankle, or with varicose veins, should NOT be given long-term support stockings unless a compelling reason has been discovered to the contrary.
- Patients with varicose veins should NOT be told that this is a cosmetic problem, and ‘fobbed off’ with the excuse that they should wait until there is a more significant problem before having anything done. There is clear evidence that up to 6% of all patients with varicose veins go on to develop Leg Ulcers in the absence of preventative assessment and/or treatment.