Although some cheap vein clinics try to justify cutting corners to keep prices down, there are some very powerful reasons to worry about doctors doing their own duplex ultrasound scans in vein clinics.
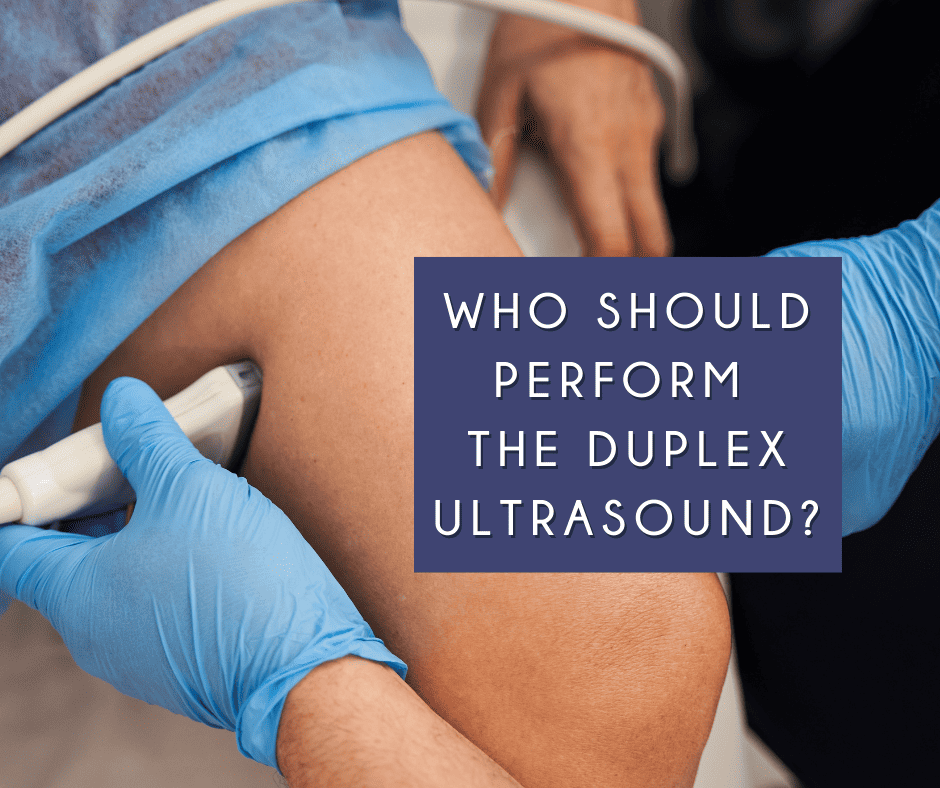
Duplex ultrasound scanning has been shown to be the best investigation to
diagnose varicose veins and also to guide the new endovenous treatments. In both situations, it is optimal for a vascular technologist or other specialist who does nothing but duplex ultrasound to perform the scan. There are many reasons for this but some of the most important are discussed here.
Hiding the results of inaccurate scans
This came to light in a case that resulted in a "specilaist" vein doctor being removed from the GMC register in 2017.
In summary, a patient came to The Whiteley Clinic concerned about varicose veins and thread veins. A duplex ultrasound scan performed by a Whiteley Clinic trained specialist vascular technologist showed no underlying varicose veins and only surface thread veins.
Although many patients will think this is good news, this patient decided to have a second opinion. They went to a different clinic and saw a doctor who specialised in varicose veins. This doctor performed their own duplex scan and told the patient that they had venous reflux in four major veins into their legs and would need endovenous laser for all of these veins.
Confused, the patient was angry and contacted Prof Mark Whiteley for an explanation. He suggested the patient go to the GMC (General Medical Council) and complain about the difference of advice so that an independent assessment could be made. The patient did this and an independent expert in venous duplex confirmed the findings of The Whiteley Clinic. It was shown that the advice that endovenous laser of the four major veins in the two legs was incorrect.
The doctor who made this error was subject to a GMC fitness to practice tribunal.
During the investigation, it was found that he had done exactly the same thing two years previously and had been reported to the GMC at that time. At that stage he had been allowed to continue to practice.
Although he had his
licence removed in 2017 and now can't practice, this whole incident has raised two major concerns.
Firstly, he had seen a great many other patients between these two cases and presumably had told all of them they needed endovenous laser when many of them would not have needed this. Because he performed his own scans, and then destroyed the veins with surgery, there is no way to go back and check any of the patients who accepted the results of his scan and underwent treatment. Hence, it is likely that many patients will have undergone unnecessary varicose vein surgery
Secondly, this opens a wider question that how do we know that other doctors are not over-diagnosing venous reflux by doing their own scan, safe in the knowledge that they are then destroying any evidence by performing the endovenous ablation?
This cannot happen at The Whiteley Clinic where all scans are performed by a specialist in venous duplex ultrasonography, reports are written and then the vein specialist doctor makes their recommendation on the results of the scan.
Prof Whiteley was so concerned about the above case that he wrote to the GMC and the Royal College of Surgeons of England, as well as several other professional bodies asking them how they monitor doctors who do their own scans from over treating patients and hiding the evidence. All of the professional bodies replied saying it was not their problem with the exception of the Royal College of Surgeons of England who have still not replied. However, unofficially, Prof Whiteley has been informed that this issue has now been raised and so things may change in the future.
Of course, if all doctors performing varicose veins were part of The College of Phlebology Venous Registry, it would soon become clear which doctors were performing more endovenous laser ablations than average. Unfortunately, most doctors are still not part of any such registry and are therefore not being transparent in their work.
NICE clinical guidelines CG 168
The
clinical guidelines on how varicose vein should be assessed and treated was published on 24th of July 2014.
In it, the guidelines clearly state that the service assessing and treating varicose veins is defined as "A team of healthcare professionals who have the skills to undertake a full clinical and duplex ultrasound assessment and provide a full range of treatment". Clearly, this is not a venous doctor sitting in a room doing their own consultation, scan and treatment!
The argument that some cheap clinics make that because they were doing this before the guidelines is fairly poor. When new guidelines come in, poor practice should be reviewed to come in line with the guidelines.
Not surprisingly, ever since Prof Mark Whiteley did the first endovenous treatment for varicose veins in the UK in March 1999, he has always used a specialist vascular technologist for diagnosing varicose veins and guiding the treatment. Subsequently, this has become an essential part of
The Whiteley Protocol.
Practice makes perfect
It is widely known to be an expert in any area, it is necessary to accrue a huge amount of experience. This is widely been promoted as 10,000 hours as a minimum. Although the exact number of hours may vary, what is very clear is to be able to perform duplex ultrasound scanning to the level needed to get a good diagnosis, the person doing the scan needs to have immense experience.
However, this is only half the story. It is also well-known that maintaining experience is just as important. Professionals who take a break away from any subject need to undergo a re-training period. Therefore, it is important to remember it is not just the training of the person doing the scan, but also what their ongoing experience is.
A doctor who spends a lot of their time in an NHS practice doing other things such as consultations, arterial surgery, other sorts of radiology, ward rounds and administration and then comes to a private clinic to see a few patients, is not going to be getting the same amount of ongoing experience as a specialist venous duplex technologist or expert who does nothing but scans every day of every week.
Therefore, any patient who is concerned should be able to ask the person doing the scan whether that is their full-time job or whether scanning is just a small part of their working week.
It is therefore, not surprising that virtually every patient who comes to The Whiteley Clinic having previously gone through an assessment elsewhere always marvels at the depth and complexity of the venous duplex ultrasound scan that they have here. Once a patient has experienced a venous duplex ultrasound scan at The Whiteley Clinic, they understand the difference between a full venous duplex ultrasound aimed at getting to all the causes of their venous problem, versus a quick scan performed by a doctor or nurse who are just checking two major veins and ignoring more complex causes of varicose veins and venous disease.
Duplex scanning guiding endovenous surgery
Many cheap vein clinics further cut corners by letting a doctor perform their own scan to guide their own endovenous surgery.
Although many doctors can scan well enough to guide themselves into one of the large veins that cause varicose veins (the great saphenous vein or the small saphenous vein), the same is not the case for the more complex veins that have been shown to be common in people with varicose veins - and even more common in people who have recurrent varicose veins!
With our international reputation for excellence, we regularly teach doctors from all around the world, at The Whiteley Clinic, how to treat patients with venous problems in the best way possible.
As 40% of patients with varicose veins have incompetent perforators, and over 60% of patients with recurrent varicose veins having the same, we have already shown that failure to treat these adequately is a potent cause of
varicose veins coming back again.
The
TRLOP technique to close perforators that was invented by Mark Whiteley and Judy Holdstock in 2001, and subsequently "reinvented" in the United States as PAPS (perforator ablation procedure) is a fiddly technique. It is necessary to be able to accurately scan a perforator that is only a few millimetres across. During the procedure, a needle needs to be introduced into the perforator and then down that needle, a device such as a laser, radiofrequency or microwave catheter in order to ablate it.
To make sure no damage is done to deep veins, this must be performed with the vein being scanned the whole time to make sure the needle and device is in the vein. This takes a minimum of three hands!
If a doctor tries to do this themselves, they end up having to drop the scanner during the procedure, meaning that they are blind during part of the procedure. This is potentially dangerous and therefore is not allowed at The Whiteley Clinic where we put patient safety first.
Whether it be perforators, other complex veins such as
neovascularisation (veins that have grown back after previous stripping surgery) or
PAVA optimal treatment is only obtained when one person is concentrating totally on the vein making sure the device is in the right place, and the other is manipulating the device itself and applying the local anaesthetic.
The suggestion this can be done by a single person means that they are either operating blind for part of the procedure which is a patient safety issue, or they are ignoring the complex veins putting their patients at risk of recurrence right from the day they are having their venous surgery.
Conclusion
It is very clear that for optimal diagnosis, optimal treatment and patient safety, venous duplex ultrasound scans should be performed by a specialised healthcare professional who spends the majority, if not all, of their working time performing venous duplex ultrasound scans. This satisfies all the problems that have been outlined above including the NICE guidelines.
Cutting corners merely to try and be cheaper puts patients at risk of having suboptimal treatment and raises the concern that inaccurate scan results are hidden, and patients may be being over-treated all of which the GMC outlined above.
At The Whiteley Clinic we have developed our protocol since March 1999, which has stood the test of time.
Of course, if other doctors and clinics are confident in their techniques and think that they are getting good results despite cutting corners, it is surprising that they have not joined
The College of Phlebology Venous Registry.
Doctors who sign up to this registry have their practice continuously monitored, with patients getting regular e-mails asking about their quality-of-life and whether their veins have come back again. Over a few years, it becomes very clear who is doing a good job and who is not.
All the doctors at The Whiteley Clinic are members of The College of Phlebology Venous Registry allowing patients confidence to know that they are happy for their results to be monitored.