



Can Microsclerotherapy Effectively Remove Spider Veins?
July 18, 2026
PUBLISHED BY

From the The Whiteley Clinica
Author conflict of interest: none.
Eur J Vasc Endovasc Surg. 2014
Sep;48(3):239-42. doi: 10.1016/j.ejvs.2014.06.044.
J Vasc Surg. 2014 Sep;60(3):796-803. doi: 10.1016/j.jvs.2014.06.102.
Eur J Vasc Endovasc Surg. 2014
Sep;48(3):239-42. doi: 10.1016/j.
ejvs.2014.06.044.
J Vasc Surg. 2014 Sep;60(3):796-803.
doi: 10.1016/j.jvs.2014.06.102.
VEITH Symposium™, New York – November 2013
DEBATE: Pre-emptive Strike on Perforators Reduces Recurrences
Mark S Whiteley
This invited commentary was published as a ‘transatlantic debate’ between 2 recognised vein experts – Prof Mark Whiteley and Prof Tom O’Donnell.
The debate was based on all of the current literature and also as of yet unpublished research from The Whiteley Clinic.
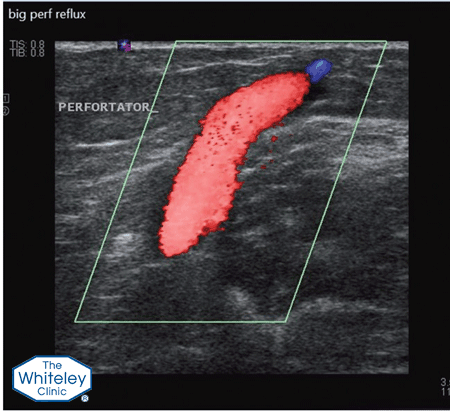
The major problem with incompetent perforating veins is that most doctors do not have the skills to treat them, as they are very small and difficult to identify. As such, rather than learn how
to treat them with techniques such as TRansLuminal Occlusion of Perforators (TRLOP – invented at The Whiteley Clinic in 2001), doctors prefer to find reasons not to treat them.
Two papers in the past had suggested that incompetent perforators become competent once the great saphenous vein has been stripped. These have been used by doctors for years as a reason to ignore incompetent perforator veins.
Unfortunately for these doctors, prize winning research from The Whiteley Clinic in 2004 showed that these studies had been flawed and, if the patients are studied for long enough, almost all of the incompetent perforators recur after stripping.
Due to our research and understanding of incompetent perforating veins, and our invention of the TRLOP minimally invasive technique of treating them, all The Whiteley Clinic patients with varicose veins or other venous problems have their incompetent perforating veins treated, if they are significant. This is one of the major reasons for the success of The Whiteley Protocol® and the very low longterm recurrence rates at The Whiteley Clinic and high patient satisfaction.
Almost all venous experts with a good research background now accept that incompetent perforators need to be treated to cure venous leg ulcers and venous skin damage. As the mechanism for venous ulceration and venous skin damage is the same as that for varicose veins, it will only be a matter of time before doctors realise that they need to treat the incompetent perforators to
reduce the risks of the varicose veins from coming back again.
Currently there is no randomised controlled trial proving incompetent perforators need to be treated as part of routine varicose veins surgery. Hence the case is neither proven nor disproven by RCT data. However as doctors, we need to treat patients by the best available techniques with the best available research to hand. This clearly shows that incompetent perforating veins should be treated to reduce recurrent varicose veins in the future.
When patients are being treated for varicose veins, incompetent perforating veins are found to be part of the venous reflux pattern in approximately half of patients. These incompetent perforating veins should be treated as part of the strategy of treating varicose veins if we want to reduce recurrences in the future.
Incompetent perforating veins are only 2 or 3 mm across and can occur virtually anywhere on the leg. As such they cannot be seen on the surface and, even using the top venous duplex ultrasound machines, are very difficult to spot. The Whiteley Clinic vascular scientists are trained to look for these and to mark them precisely. Incompetent perforating veins are often ignored by doctors who do their own scans and who do not find them.