Varicose Veins Treatments
Varicose Veins Treatment, Surgery & Removal
How we treat your varicose veins differently

To achieve our aim of removing the underlying cause of the varicose veins as well as the external visible signs, we follow The Whiteley Protocol®. It is a co-ordinated system of examination, investigation and diagnosis leading to an individually-tailored treatment plan, bespoke for every patient.
After your assessment with one of our specialist Vascular Scientists, you will be given a full breakdown of the bespoke treatment plan recommended for you, which may include a number of options and procedures, that are all available at The Whiteley Clinic.
All of our procedures are performed under local anaesthetic as ‘walk in, walk out’ surgery. This means that, unless there are any exceptional circumstances, patients should be back to work and back to relatively normal activities the day following their treatment.
Because we develop personalised treatment plans that are appropriate to each individual patient, we are unable to give exact prices for a proposed suite of procedures until one of our specialist Vascular Scientists has performed the extensive venous duplex ultrasound investigations.
In the UK, many doctors still regard varicose vein surgery as ‘simple’, offering a set price for treatment and only using quick scans for diagnosis – often performed by the doctor themselves. This ‘one size fits all’ treatment method is one of the reasons that recurrence rates are so high in many practices, hospitals and clinics. The Whiteley Clinic approach varicose vein treatments in a different way, all our treatments are based on our award-winning research.
Our goal isn’t just treatment of varicose veins, its treatment with the lowest possible chance of recurrence and the highest patient satisfaction – even in the long term.
For a first hand account of patients we have successfully treated, please see our testimonials and video testimonials
Leg Varicose Veins
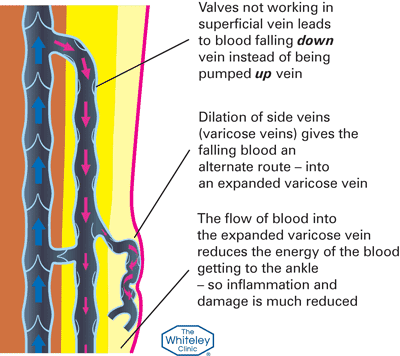
Varicose veins are easily recognized in many people as bulging leg veins on standing or sitting. Unlike other lumps on the legs, when lying down, varicose veins will empty and disappear. This is because the veins are filling from underlying veins that have lost their valves, and blood falls down the veins by gravity. This blood falling the wrong way is called “venous reflux”. This venous reflux fills the surface veins or “tributaries”. When this has been going on for a long time, the walls of the surface veins can stretch, causing the visible varicose veins.

In many cases, the blood refluxing down the leg veins on standing or sitting also causes a colour change at the ankle. The skin can appear more red or blue. When lying down and lifting the leg, the blood drains out and the colour goes back to normal. This simple test can be used at home to see if you might have varicose veins or “hidden varicose veins” deeper inside the leg.
Hidden varicose veins
About 15-20% of adults have varicose veins visible on the legs. However, what is harder for many people to understand is that another 9-20% of adults have “hidden varicose veins” that cannot be seen on the surface. If varicose veins were only “cosmetic”, then this would not be a problem. However, as it is venous reflux that causes varicose veins and hidden varicose veins, this will cause the veins to deteriorate until the reflux is treated. Indeed, research shows that about 1 in 20 (5%) of people with varicose veins will deteriorate each year if they don’t have their veins treated.
As noted above, for centuries the medical profession has focused on the bulges themselves as the problem, often thinking the bulging ‘varicose veins’ are the problem. However, research in recent decades has shown that the veins appearing on the surface only do so because the veins deeper inside the leg have lost their essential valve function, allowing blood to flow the wrong way down the veins – venous reflux. So the traditional kind of treatment – still offered by some practitioners – that is directed solely at the veins seen on the surface, without either investigating or treating the underlying cause, is bound to fail.
The problem is worsened further by the fact that, until recently, medical opinion held that only two principal veins could become ‘varicose veins’. Many doctors still only check and treat these 2 veins! However, studies – including research conducted by The Whiteley Clinic – has now shown that the condition can affect a large number of different veins such as incompetent perforator veins and pelvic vein reflux. If a doctor doesn’t have access to the correct diagnosis from a detailed scan in the first place, he or she is unlikely to be able to perform a complete treatment that will minimize the risk of recurrence.
New techniques to treat varicose veins
A single doctor working in a room by themselves, and doing their own scan is not able to check all of these veins and also be an expert in treating them. Hence NICE – The National Institute of Health and Care Excellence recommends that patients with varicose veins are referred to teams of professionals working together, and able to perform duplex ultrasound scans and ALL of the new techniques needed to treat varicose veins.
This was recognized by Mark Whiteley in 1998, 15 years before the NICE Guidelines, and is the reason why The Whiteley Clinic have always worked in such teams. At the The Whiteley Clinic we have always placed great emphasis on performing comprehensive diagnostic tests and scans – based on a foundation of Duplex Ultrasound Scanning (Link to internal WC page of Duplex Ultrasound – in advance of the development of any treatment plan. This is a key part of our strict adherence to The Whiteley Protocol® and it ensures that all of our investigations are performed by independent experts who specialise in Duplex Ultrasound examination of the veins.
You can compare our approach with the trend in recent years where doctors in ‘cheaper’ varicose vein clinics perform their own scans to try to keep prices down – despite the recommendations by NICE. This is a false economy as it has been shown that missing incompetent perforating veins or pelvic vein reflux are two of the commonest reasons that varicose veins come back after treatment.
This contrasts with our own results showing that after 15.4 years of follow-up, the risk of varicose veins recurring after treatment at The Whiteley Clinic with The Whiteley Protocol®, is the same per year as people who come from a family with varicose veins running in it, but who don’t have varicose veins themselves. Hence, it is impossible to get a lower risk of recurrence than we achieve.
But then, as with so many things in life, cutting corners to reduce costs usually means a reduction in standards, which in terms of varicose veins means varicose veins come back again quicker and more often. Put simply, it is a clear case of “Buy cheap, buy twice”!
Common Myths About Varicose Veins
Up to 40% of the adult population has varicose veins or hidden varicose veins and because it’s a common condition, there’s a lot of ‘conventional wisdom’ surrounding the topic, which leads people to believe that they understand the facts. However, research over the last decade – much of it conducted by The Whiteley Clinic – has revealed that many of the ‘facts’ concerning varicose veins are actually ‘myths’…
Women get varicose veins more often than men
Many early studies by doctors seeing patients who came to ask for treatment for their varicose veins suggested that women were more likely to suffer with varicose veins than men. But we now know that this is a varicose veins myth. It’s simply the case that women are more likely to do something about varicose veins, and therefore the female gender represents the higher statistical proportion of patients.
Further studies have subsequently shown that varicose veins occur roughly in the same proportions in both men and women, but that men are much more likely to ignore their symptoms.
Pregnancy causes varicose veins
Research published at the end of the 1990’s suggested that when patients were scanned first before and then after pregnancy, those women who had thought they had developed varicose veins during the pregnancy had actually already had hidden varicose veins which were visible on their pre-pregnancy scan.
Varicose leg veins are not actually caused by the pregnancy (although pre-existing varicose veins will worsen during pregnancy due to the increase in blood volume and changes in hormones). However, there is a specific varicose vein that is only found in women who have both been pregnant and had a normal delivery, and that is vaginal varicose vein or vulval varicose vein. This important condition is covered elsewhere on this website under pelvic congestion syndrome, vaginal and vulval varicose veins and pelvic vein embolisation.
Women should wait until they’ve had their children before getting their veins fixed
We know that varicose veins swell during pregnancy and this causes discomfort. In addition, we also know that the risk of phlebitis in varicose veins is much higher at the end of a pregnancy and immediately after the pregnancy. For that reason, the advice offered by The Whiteley Clinic (and which we would recommend all doctors and nurses to their patients) is to have varicose veins treated before the pregnancy itself, provided of course that their chosen clinic uses the latest techniques and can claim a level of positive results equivalent to those obtained by using The Whiteley Protocol®.
Crossing your legs causes varicose veins
In years gone by, following surgery or after a long hospital stay, patients often developed deep vein thromboses (DVT) in the leg veins. In some cases, the clot could break off and travel to the lungs causing a pulmonary embolism (PE) that could prove fatal.
Of course, nowadays patients are given special stockings and also injections of subcutaneous heparin to reduce this risk. However, before these measures were available and before the problem was fully understood, nurses and doctors used to tell patients not to cross their legs, thinking that it was the pressure on the calf that caused the DVT.
This varicose veins myth has become so prevalent that most people have forgotten that it used to be a DVT-related ‘truism’ and simply assume that it is sound medical advice to stop the development of varicose veins.
The truth is… it’s another varicose veins myth!
If simple pressure from crossing one’s legs really did cause venous problems, then we would all be constantly getting DVT or varicose veins every time we sat down or did anything that put any pressure on the legs. You can rest assured that we humans have evolved in such a way that the important veins of the legs are protected from the points of pressure during such movements as sitting, kneeling… and, of course, crossing legs.
Having hot baths causes varicose veins
One of the major roles of our veins is to regulate the body’s temperature. Veins work in co-operation with arteries and capillaries to control the flow of the blood to the skin, allowing heat to be lost or retained.
Having a hot bath causes the capillaries to dilate, making the skin go characteristically red. However this is a normal reaction and as soon as you get out of the bath, the capillaries start to contract again and everything goes back to normal.
The development of varicose veins has nothing whatsoever to do with this normal dilation of capillaries and small veins. Otherwise, we’d develop varicose veins not just in just one leg or one part of one leg, but all the way up to the waist… and on both legs, depending on the depth of the bathwater!
The only time The Whiteley Protocol® calls for hot baths to be avoided is following sclerotherapy treatment for varicose veins. We advise patients not to go into hot weather or hot baths for at least 14 days after treatment as the effect of dilating veins in the process of healing can result in increased blood flow into dying veins, which in turn can result in brown stains on the skin.
Varicose veins are a sign of poor circulation
Now there’s an all-encompassing statement! And utterly without basis in fact. Varicose veins have no effect at all on circulation, nor do they increase the risk of stroke or heart attack or cause cold fingers or toes.
Many non-medical people not only consider veins to be the same as arteries, but also have a shaky understanding of their role in circulation. Although blood does go through the arteries and then into the veins during normal circulation, the two halves of the system are very different.
The arterial side of the circulation system is ‘high pressure’ and problems on this side result in strokes, heart attacks, aneurysms and ‘dead legs’ requiring bypass surgery or amputation.
The vein (also known as ‘venous’) side of the circulation system, the blood is ‘low pressure’ and problems on this side result in varicose veins, clots (such as DVT), thrombophlebitis, swollen ankles and venous leg ulceration.
Many people say they have poor circulation if they have cold fingers or toes; however in the vast majority of people, this is a condition called Raynaud’s Syndrome which is an abnormal contraction of the capillaries in the fingers or toes, usually caused by exposure to cold or as a result of other factors such as smoking.
Varicose veins are only cosmetic and can safely be left alone
Hopefully if you have read the other pages in this section on varicose veins, you already know that this statement is not only wrong on both counts but can also be dangerous in encouraging complacency.
There are people with thread veins and spider veins who have a Duplex Ultrasound scan which shows that they do not have any underlying hidden varicose veins or venous reflux. Yes, for these lucky people, varicose veins are indeed just a cosmetic problem.
And there are people with very small green veins or very small varicose veins who, following their scan, are shown to not have any underlying hidden varicose veins or venous reflux. Once again, for these people, varicose veins are only a cosmetic problem.
However, for the majority – yes, the majority! – of patients who come to see us, a Duplex Ultrasound scan will find a more serious and hidden underlying varicose vein problem of which they were quite understandably unaware when they were simply looking at bulging veins on the leg.
The National Institute of Health and Clinical Excellence (NICE) has recognised that if anybody has varicose veins (and suffers any symptoms from them) they should be referred to a specialist vascular service such as The Whiteley Clinic. NICE endorses and encourages proper investigation using venous Duplex Ultrasound, followed by treatment using the latest techniques.
And, no, varicose veins cannot safely be left alone. They don’t get better by themselves, they will always deteriorate if left alone, and (for at least 3 to 6% of people) they very well may go on to cause venous leg ulcers. And for an even higher proportion of patients, leaving their veins untreated may lead to a worsening of marginally less serious symptoms including skin damage, thrombophlebitis, venous eczema or swollen ankles.
There’s no point in operating on varicose veins as they always come back
Up until March 1999, this was probably true in all vein practices. And amongst those clinics that continue to rely on the outdated (and frankly barbaric!) technique of stripping vein, yes, there is a definite likelihood of the problem recurring. This has been proven by a series of prize-winning research projects undertaken by The Whitely Clinic and published in the British Journal of Surgery (2007) and in the specialist venous journal ‘Phlebology’ in 2014.
What changed in the Spring of 1999 was that Professor Mark Whiteley of The Whiteley Clinic introduced into the UK a technique called ‘endovenous laser ablation’ for varicose veins.
Research has shown that varicose veins closed using Mark Whiteley’s ground-breaking endovenous laser ablation (or as NICE calls them ‘endothermal techniques’) as part of The Whiteley Protocol do not come back again after treatment in the vast majority of patients. Indeed, the only recurrence after treatment tends to be normal veins that have also subsequently deteriorated and lost valve function.
You have to walk 5 miles a day after varicose vein treatments
This particular varicose veins myth came about as a result of an observation once made by one of the pioneering heroes of varicose vein surgery, a very charismatic Irish surgeon called Professor George Fegan. The Professor mentioned in conversation that a patient who had walked home after sclerotherapy went on to enjoy the best post-surgical outcome that he had ever seen. This story was passed on, repeated, and interpreted by generations of vein specialists until his supposed recommendation for patients to walk 5 miles every day post surgery passed into folklore as a piece of ‘best practice’…
There certainly is some truth that walking after any vein treatment reduces the risk of deep vein thrombosis and is therefore a good idea. But at The Whiteley Clinic, we don’t encourage our patients to hike for 5 miles every day!
The venous surgery that we perform using local anaesthetic is ‘ambulatory’ surgery, meaning patients do indeed literally walk in and walk out, enabling them to get straight back to everyday life and normal activities.
Yet another varicose veins myth!
Standing for long periods of time causes varicose veins
In the past there have been many research papers published showing that severe varicose veins are more common in people whose professions involve them standing up for a long period of time, such as hairdressers, teachers and surgeons. In particular, on its website, the facts cites the avoidance of standing up for long periods as part of its suggested six month programme of self-care at home before it will consider treating varicose veins!
However, the most recent research has shown that the standing in fact does not cause varicose veins; it merely makes the condition worse if varicose veins are present.
At The Whiteley Clinic, we recommend that anyone who stands for long periods of time and suffers with varicose veins, or who has any signs or symptoms, should have them treated with the latest endovenous techniques to stop complications and prevent further deterioration.
In the past, particularly in the case of NHS treatment, patients have been advised to wear compression stockings or graduated pressure stockings as an alternative or a precursor to surgery. This has now been shown by studies and also the National Institute of Health and Clinical Excellence Guidelines (NICE) to be substandard advice. Compression stockings or graduated pressure stockings can be used whilst waiting for varicose vein treatment, or as part of the treatment following sclerotherapy, but they are not, in themselves, a treatment for varicose veins.
You need 14 days off work after varicose vein surgery
As mentioned above, the world of venous surgery changed in March 1999 when Professor Mark Whiteley of The Whiteley Clinic introduced into the UK a technique called ‘endovenous laser ablation’ for varicose veins.
Prior to this, ‘varicose vein stripping’ was the best treatment option for varicose veins, and most patients did indeed need 10 to 14 days off work to recover from the pain and bruising of the surgery.
Since the advent of endovenous surgery techniques, patients having varicose vein surgery following The Whiteley Protocol® are able to walk normally the following day and return to normal life that day.
Varicose Veins run in families
Now this is the one varicose veins myth that is actually based on fact.
There is a strong familial link and the more relatives you have with varicose veins, the more likely you are to have them even if they are hidden varicose veins.
The link cannot be termed as solely genetic as patients often only have varicose veins on one leg and not the other, or in one vein in the leg and not another. If there were to be a very strong genetic link, all of the veins would be affected at the same time. As such there must be other factors that work in conjunction with the genes to make people more susceptible to having varicose veins.
Please click on individual procedures for more information:
- Sonovein® HD(Echotherapy Treatment)
- Microwave Varicose Vein Treatment (EMWA)
- Endovenous laser ablation (EVLA)
- Radiofrequency ablation (RFA) of varicose veins
- TRansLuminal Occlusion of Perforators (TRLOP)
- Foam Sclerotherapy – ultrasound guided foam sclerotherapy (UGFS)
- Glue (Venaseal) – glue treatment of varicose veins
- Phlebectomies – Ambulatory phlebectomies
- Microsclerotherapy
- Pelvic Vein Embolisation (PVE)
- MOCA (Clarivein)