Varicose vein research laboratory
February 19, 2026
Radiofrequency ablation (RFA) and endovenous laser ablation (EVLA) of varicose veins are the NICE recommended ways of treating varicose veins (see NICE CG168). However, as this case shows, they only work if used appropriately and guided by expert venous duplex ultrasonography. This patient came to The Whiteley Clinic
recently for help with his severe recurrent varicose veins and skin damage to the lower leg.

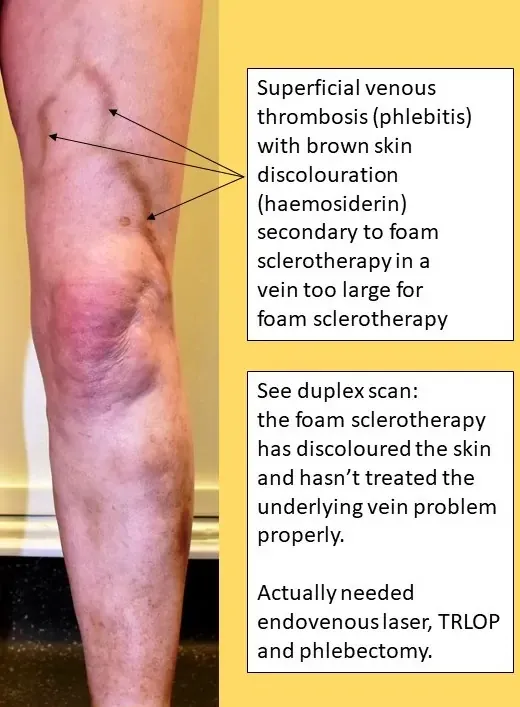
Recurrent Varicose Veins after "Successful" Radiofrequency Ablation of Great Saphenous Vein performed elsewhere
He has had worsening of varicose veins in his left leg over several years. Initially, he saw only varicose veins. However, he left them alone and, not surprisingly, they deteriorated. Firstly he started getting swelling around the ankle after a day of standing. This then worsened to red stains, followed by brown stains, around his lower leg and ankle. The brown stains on his lower leg show the severity of the vein problem he has. This is called "haemosiderin" staining. It is classified as CEAP C4 skin damage. The next stage of skin damage after this is a venous leg ulcer. Two years ago, his GP sent him to a local vascular surgeon. As with most vascular surgeons in the UK, this surgeon spent most of his time doing arterial surgery and did not specialise in veins. The patient says that he had a quick five-minute scan and was told that he had a problem with his "long saphenous vein". To a vein specialist, this rings alarm bells as the "long saphenous vein" was renamed the great saphenous vein in 2001. He underwent radiofrequency ablation (RFA) of his great saphenous vein in 2015 with virtually no change in his veins at all. He said that initially, a few lumpy veins in the thigh seemed to disappear, but overall the leg continued to deteriorate. He went back to his surgeon who suggested he could have a more extensive operation under general anaesthetic. Rather than undergo this, he decided to come for a second opinion to The Whiteley Clinic.
As with all of our patients, our approach was by using The Whiteley Protocol. The patient had a full consultation with a The Whiteley Clinic trained consultant venous specialist and then underwent an extensive venous duplex ultrasound scan by a Whiteley clinic trained clinical vascular scientist (vascular technologist). This duplex ultrasound scan showed that the previous radiofrequency ablation (RFA) had been successful in closing the top of the great saphenous vein. However, the mid part and bottom of the great saphenous vein had been left open and incompetent. But far more importantly, a massive and incompetent anterior accessory saphenous vein had been completely missed and was still causing major venous reflux and varicose veins in the thigh (clearly visible on the photograph). In addition, two incompetent perforators were underlying the brown staining of the skin, causing inflammation in the veins and skin of the lower leg. Fortunately, this is all curable by The Whiteley Protocol. He will be able to have local anaesthetic treatments on two occasions as follows: Stage I: endovenous laser ablation anterior accessory saphenous vein and remnant of the great saphenous vein + TRLOP closure of perforators + phlebectomies Eight weeks after that he will then have: Stage II: ultrasound-guided foam sclerotherapy to veins remaining patent under the damaged skin in the lower leg. This will cure his varicose veins and will stop him deteriorating to leg ulcers. Over time, the brown staining will start to improve.
There are several reasons as to why patients do not necessarily get the optimal treatment for varicose veins and other venous conditions in the UK. Firstly, varicose veins are mainly done by "vascular surgeons". Most vascular surgeons spend the majority of their time treating arterial problems - abdominal aortic aneurysms, leg bypass grafts or carotid arteries. This leaves precious little time to be specialists in veins. The few of us who specialise in veins, such as the experts at The Whiteley Clinic, should be called Consultant Phlebologists. However, this speciality does not currently exist in the UK and so consultant vein specialists from a surgical background are still called "vascular surgeons". This makes it very hard for patients to know if they are seeing a vein specialist or not. Secondly, traditional teaching is that varicose veins only arise from either the great saphenous vein or the small saphenous vein. Those of us specialising in venous surgery know that this is not the case and that varicose veins that can go on to cause skin damage and leg ulcers can arise from:
as well as several other rarer causes. Therefore if a doctor does their own quick scan or uses a general scanning department, and the scan only looks for the great saphenous vein and the small saphenous vein, it is not surprising that some incompetent veins are missed. The NICE clinical guidelines suggest that people treating varicose veins should work in multidisciplinary teams as we do at The Whiteley Clinic. In this way, scans can be performed by expert technologists who do nothing but venous scanning and therefore rarely miss the underlying causes for varicose veins and other venous diseases. As the scans often take 30 to 40 minutes each, it is not surprising that when doctors do their own scans, they do not have this much time and frequently miss the causes of varicose veins. Research presented at the Veith Symposium in New York in 2014 showed that when doctors who also operate do their own scans, they can miss 30% of the relevant veins. Thirdly, most doctors in the UK still do not look for or treat incompetent perforating veins. Although there is now clear evidence that venous leg ulcers heal better and faster if incompetent perforating veins are treated, doctors are slow to accept that this same problem can be found in patients with other venous conditions. It is illogical and the arguments have been published from The Whiteley Clinic in international journals in Europe and America.
At The Whiteley Clinic, we have addressed the issues that commonly result in poor results from varicose vein surgery. We specialise in veins and venous conditions and work as a multidisciplinary team with doctors, clinical vascular scientists (vascular technologists) and nurses who all specialise in venous disease. All of our doctors, clinical vascular scientists (vascular technologists) and nurses are trained in The Whiteley Protocol to ensure a uniformity of excellence in veins. We do not ever use locums or agency staff. We perform our own research ensuring that each pattern of veins gets the appropriate combination of treatments to get the very best results. This approach and the resultant combination of treatment is called "The Whiteley Protocol". We regularly audit and publish our results showing that our attention to detail gives us the lowest possible risk of recurrent varicose veins in the future. In this way, we make sure that we do not get patients like this patient presented above, who only had one of his four incompetent veins treated.