This lady with leg vein problems came to the specialists at The Whiteley Clinic for treatment. She had
varicose veins and
thread veins (spider veins) of her legs.
The patient who was in her mid-thirties had noticed the veins for many years but had not thought to get them treated. Over time some areas had got much darker and had gone brown.
She had two children and during pregnancy, had noticed the varicose veins appearing at the top of her legs. These were on the inside of her upper thigh, next to her vulva and vagina. These are called “para-vulval” – or next to the vulva.
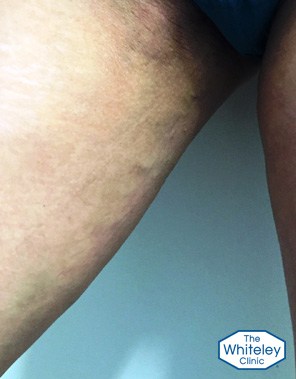
As can be seen by the pictures, the legs look relatively normal when viewed from the front. However there are two very brown areas on the outside of the left calf, with a very dark brown stain on the left calf muscle at the back.
There is a very impressive varicose vein with thread veins and brown stains, snaking diagonally across her right thigh at the back from the area of the vulva to the outside of the knee.
Finally, checking sides of her thighs at the very top, she had very clear varicose veins in the para-vulval region on both sides, which are easier to see on the left.
Varicose veins arising from pelvic varicose veins
Traditionally most people, including doctors and nurses, had thought that leg varicose veins are confined to the legs.
Research from The Whiteley Clinic has shown that one in seven
(14%) women with varicose veins actually have them arising from varicose veins in the pelvis. This rises to one in five
(20%) of women who have had children and who have leg varicose veins.
This is very important when it comes to trying to stop them coming back after treatment. If they are coming from varicose veins in the pelvis, and a doctor only investigates and treats leg veins, these will come back again after treatment. This is one of the most common causes of recurrent varicose veins and is also a major cause of patients and doctors thinking that "varicose veins always come back" - which is not true if they are treated properly!
This lady is an excellent example of the problem. She clearly has varicose veins, thread veins and also brown stains of the skin caused by varicose veins. However the duplex ultrasound scan shows that all but one of her main leg veins are completely normal, and all of the visible varicose veins are arising from pelvic varicose veins.
If this lady had her leg veins treated, regardless of which technique was used, she would only get them back again in the future. She needs to have her pelvic veins treated with
pelvic vein embolisation before she can get successful treatment of her leg veins.
Brown staining (haemosiderin) due to old phlebitis

The dark brown stains on the legs come from a complication called "phlebitis".
Phlebitis means an inflammation of the veins.
In veins that have become varicose, the blood does not flow in the normal direction. Therefore, in some patients the blood clots. When this happens in veins near the surface, the blood clot or "thrombus" inflames the vein and the overlying skin.
This inflammation causes the area to go red and lumpy in the short term. However as this settles down, iron in the blood caught in the thrombus leaches out into the skin. Because iron is toxic to the skin, the body surrounds the iron with protein following a brown pigment called haemosiderin.
Whilst the varicose veins remain, phlebitis will keep occurring causing further brown staining. In areas where there is already brown staining, even darker brown pigments will appear.
The only treatment for this is to treat the underlying problem first, preventing any more phlebitis, and then the brown staining will slowly settle.
CEAP score of C4 - skin damage due to varicose veins

The severity of varicose veins is graded by the CEAP score. This is explained in more detail on our
self-assessment page.
This lady has thread veins (telangiectasia) which means she is at least a C1. She also has varicose veins, raising her grading to C2. However because she has had recurrent phlebitis, which has resulted in skin damage, she is graded as C4.
By the
National Institutes of Health and clinical excellence (NICE) clinical guidelines she has varicose veins with skin damage and therefore requires investigation with duplex ultrasound scan by a team of specialists, and treatment of her varicose veins.
Unfortunately, NICE currently does not recognise pelvic varicose veins and so this is where treatment and research at The Whiteley Clinic is ahead of the clinical guidelines by NICE.
If she is treated by NICE guidelines alone, and the pelvic veins were not investigated and treated, she would end up getting her veins coming back year after year.
Hopefully it will not be long before NICE catches up with what this lady requires and a cure the condition.
Treatment for this patient
Treatment for this patient, as with all patients coming to The Whiteley Clinic, is determined by
The Whiteley Protocol®.
She will undergo a
transvaginal duplex ultrasound scan which has been shown to be the gold standard test for pelvic vein reflux and pelvic varicose veins.
Once the problem veins in the pelvis are identified, these will be treated by pelvic vein embolisation procedure.
Once the pelvic varicose veins have been treated, we can then treat the leg varicose veins safe in the knowledge that they have the lowest chance of ever coming back again.
Click on
The Whiteley Protocol® for more information.