



Can Microsclerotherapy Effectively Remove Spider Veins?
July 18, 2026
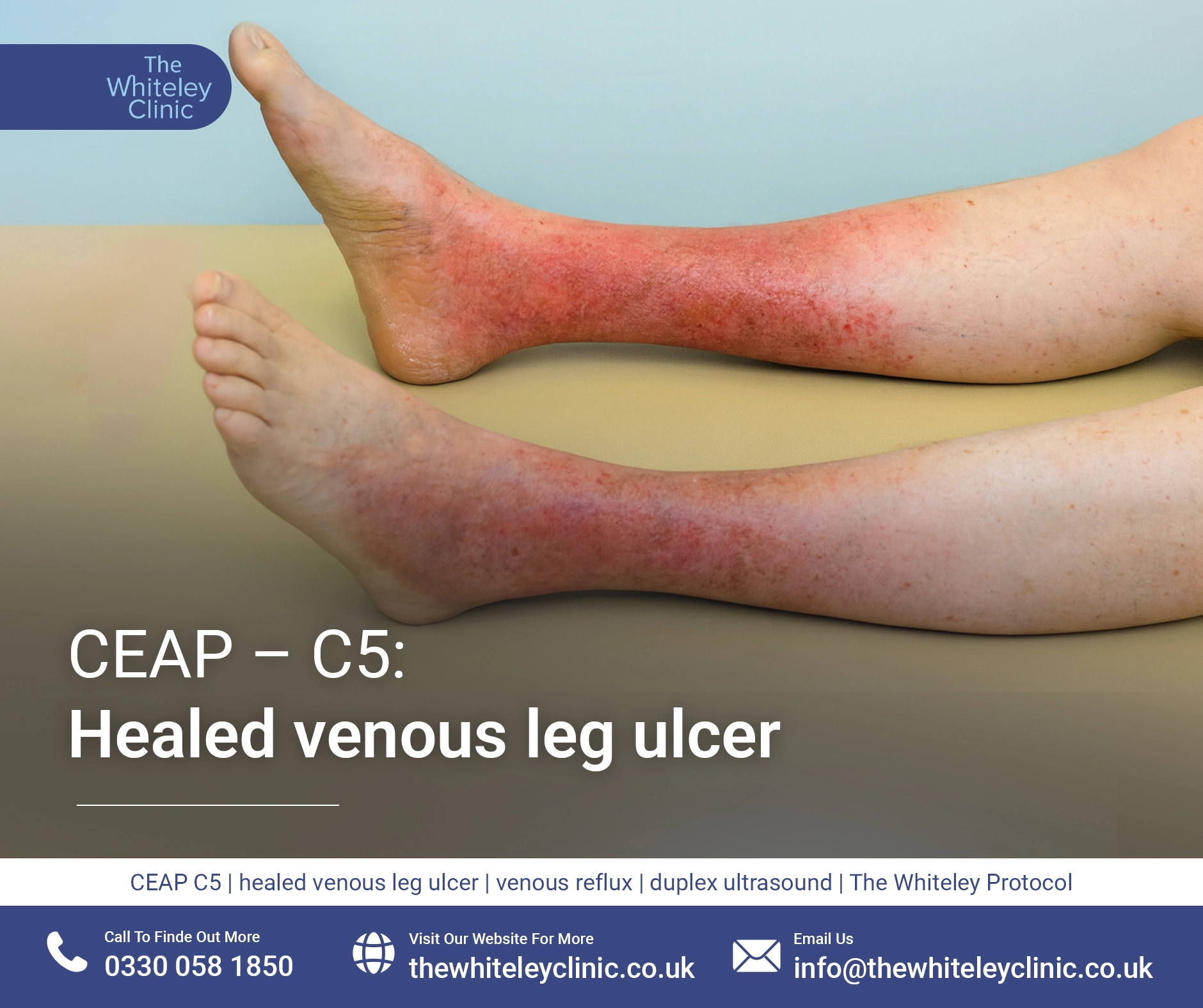
In the CEAP scale of disease severity, CEAP C5 is a healed venous leg ulcer. This seems to be illogical as CEAP C4 is skin damage at the ankle due to varicose veins and when this progresses to a leg ulcer, it becomes CEAP C6. It is impossible to get to CEAP C5 if you have not already had an active leg ulcer CEAP C6. In other words, it is impossible for a patient to progress from CEAP C4 (skin damage) to CEAP C5 (healed venous leg ulcer) unless they have already jumped to CEAP C6 (active venous leg ulcer) first.
Therefore this shows that the CEAP classification of clinical severity from varicose veins and “hidden varicose veins” (venous reflux) is not a progression from C1 to C6 but is merely a clinical grade that can be given on the day.
The fact that a healed venous leg ulcer is probably less of a clinical problem than an active venous leg ulcer supports the fact that CEAP C5 is a healed leg ulcer and CEAP C6 is an active leg ulcer. Therefore, provided everyone understands that the scale is not a linear progression that a patient follows, then it is still a useful scale.

Venous leg ulcer healed by endovenous treatment using The Whiteley Protocol® – CEAP-C5
A healed venous leg ulcer usually shows the skin damage around the ankle or lower leg typical of CEAP C4, and the patient or their carers/relatives will tell you that there was an open ulcer in that area previously. In most cases, there is a scar from the previous leg ulcer which is a different colour to the CEAP C4 surrounding it.
If the area of healed ulcer is not surrounded by skin changes typical of CEAP C4, then this would put the diagnosis in doubt. There are other causes for leg ulcers although venous leg ulcers are by far the most common form of leg ulcer.
It is essential to know that a healed venous leg ulcer is highly likely to keep coming back again if the underlying vein problem has not been treated. Compression treatments for venous leg ulcers are never a long-term treatment. They may temporarily heal a venous leg ulcer but without treating the underlying venous problem, they will almost always come back again.

Healed varicose leg ulcer 6 weeks prior folowing endovenous treatment using The Whiteley Protocol® – CEAP-C5
The underlying cause of a CEAP C5 healed venous leg ulcer is almost always venous reflux secondary to varicose veins or “hidden varicose veins” and so the condition is almost always curable.
Sometimes, a CEAP C5 healed venous leg ulcer can be due to deep vein problems such as deep vein reflux secondary to severe all recurrent deep vein thrombosis (DVTs) – which is called post thrombotic syndrome (PTS) – or can be due to narrowing or blockage of the veins in the upper leg or pelvis, stopping the blood from flowing out of the leg veins efficiently.
Therefore, the usual underlying cause of a healed venous leg ulcer is venous reflux related to varicose veins or “hidden varicose veins”. This reflux is usually in the great saphenous vein, small saphenous vein or from incompetent perforators – or of course any combination of these. All of this reflux can be treated using the techniques researched at The Whiteley Clinic, but none of these refluxing veins are treated by compression bandaging, graduated compression stockings or support stockings. When such techniques are used, there is a temporary improvement of the reflux due to the pressure. This can lead to a temporary healing of the leg ulcer, resulting in a CEAP C5 healed leg ulcer. However, if the underlying veins have not been treated, once the compression is removed, it is only a matter of time before the leg ulcer returns.

If you have a CEAP C5 healed leg ulcer because you previously had a CEAP C6 active leg ulcer and then underwent endovenous treatment at a specialist unit such as The Whiteley Clinic, then you do not need to do anything else because you are cured and it is highly unlikely that your leg ulcer will ever return. Please see our results of treating venous leg ulcers over 12 years in ncbi website.
However, if you have a CEAP C5 healed venous leg ulcer because of compression bandaging, dressings, elevation of the leg compression stockings, without any investigation or treatment of your underlying veins, then unfortunately you will almost definitely get your leg ulcer back again. This is because the underlying problem that cause the ulcer in the first place has not been treated. As soon as the compression is released, the same problem occurs and the ulcer breaks down once again.
Therefore, if you have a CEAP C5 healed venous leg ulcer and have not had venous duplex ultrasound scan of your veins in a specialist vascular service such as The Whiteley Clinic, then you need to have have this done as soon as possible.
Indeed the National Institute of Health and Clinical Excellence (NICE) clinical guidelines CG 168 published in July 2013 are very clear on this fact. Anyone who has a healed leg ulcer should be referred to a vascular service for a specialist venous duplex ultrasound scan and consideration of endovenous surgery to ensure that the healed ulcer becomes a cured ulcer and does not return again.
See here: nice.org.uk
The Whiteley Clinic satisfies all of the criteria in this NICE recommendation, as all patients see a multidisciplinary team, having a venous duplex ultrasound scan performed by a specialist vascular scientist and then being reviewed by a specialist consultant trained in The Whiteley Protocol® and able to provide all of the endovenous treatments that may be required. An individual doctor doing their own scans and treatments as is often found in cheap vein “clinics” does not comply with these NICE guidelines.
Anyone with a CEAP C5 healed venous leg ulcer should ensure that they have the correct investigation and treatment to prevent the CEAP C6 leg ulcer from recurring in the future.