Hidden Varicose Veins
Hidden varicose veins are a common but often overlooked form of venous disease. Unlike traditional varicose veins, they do not produce visible bulging veins on the surface of the legs. However, they can still cause significant symptoms, including aching, heaviness, swelling, skin damage, and even venous leg ulcers. Hidden varicose veins develop when faulty vein valves allow blood to flow in the wrong direction, creating a condition known as venous reflux. In many cases, patients experience symptoms for years before receiving an accurate diagnosis because their legs appear normal. Understanding hidden varicose veins is essential for identifying the true cause of unexplained leg symptoms and preventing long-term complications.

Understanding the Veins in the Legs
To understand hidden varicose veins, it is important to understand how the venous system works.
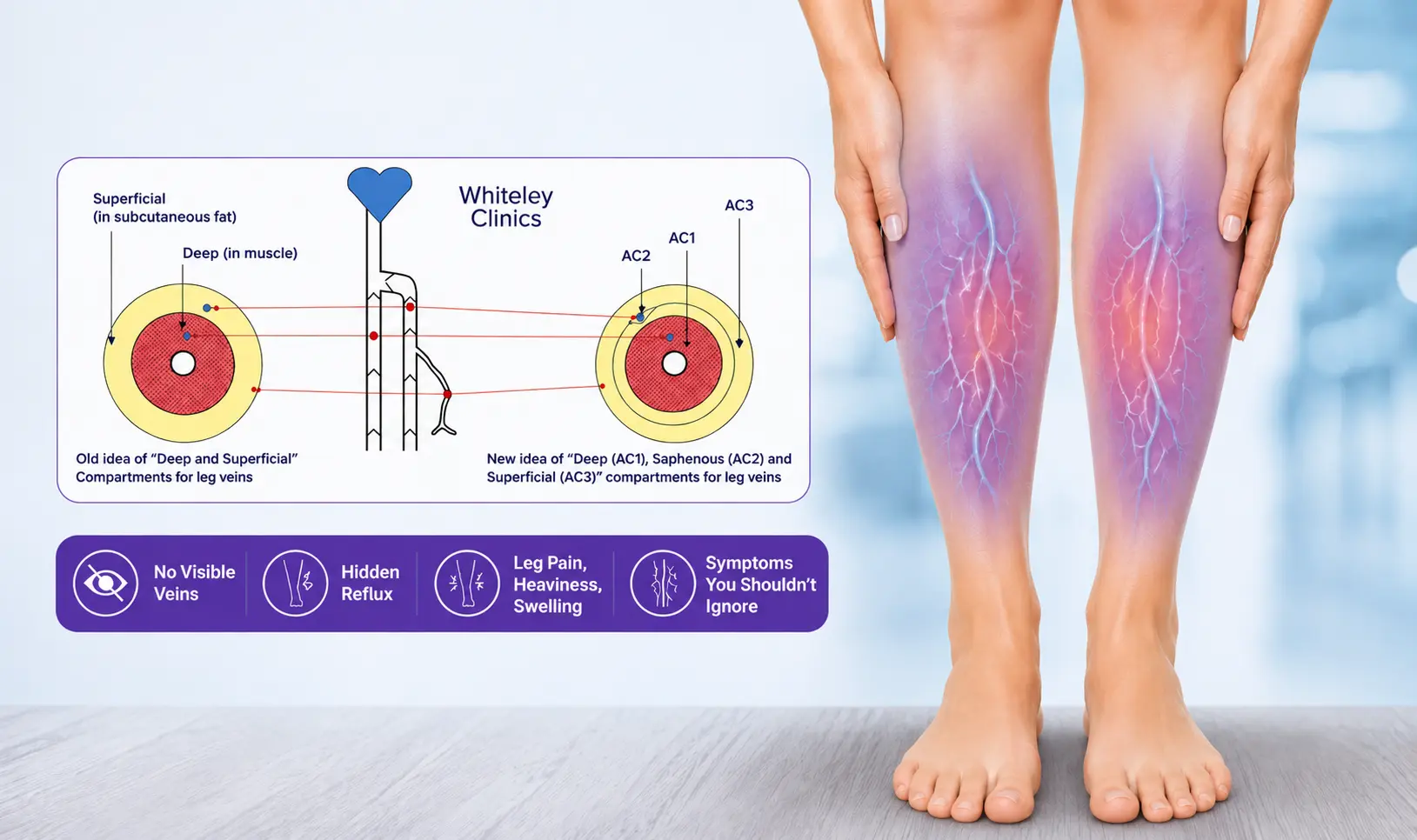
Many healthcare professionals still classify leg veins as either deep veins or superficial veins. Deep veins lie within the muscles, while superficial veins sit within the fatty tissue beneath the skin.
This traditional description is only partly accurate, as modern venous anatomy presents a more detailed framework.
The deep veins form Network One (N1) and are located within Anatomical Compartment One (AC1). The majority of venous blood is directed back to the heart through these vessels.
The main superficial trunk veins form Network Two (N2). These include:
- Great Saphenous Vein (GSV)
- Small Saphenous Vein (SSV)
- Anterior Accessory Saphenous Vein (AASV)
The old names are the long saphenous vein and the short saphenous vein. However, these names were changed in Europe in 2001-2 and America in 2004-5. Healthcare professionals using these old terms are well over a decade out of date.
These veins are often called truncal veins because they act as the main channels that return blood to the deep venous system. Importantly, they lie within Anatomical Compartment Two (AC2), making them invisible from the skin surface.
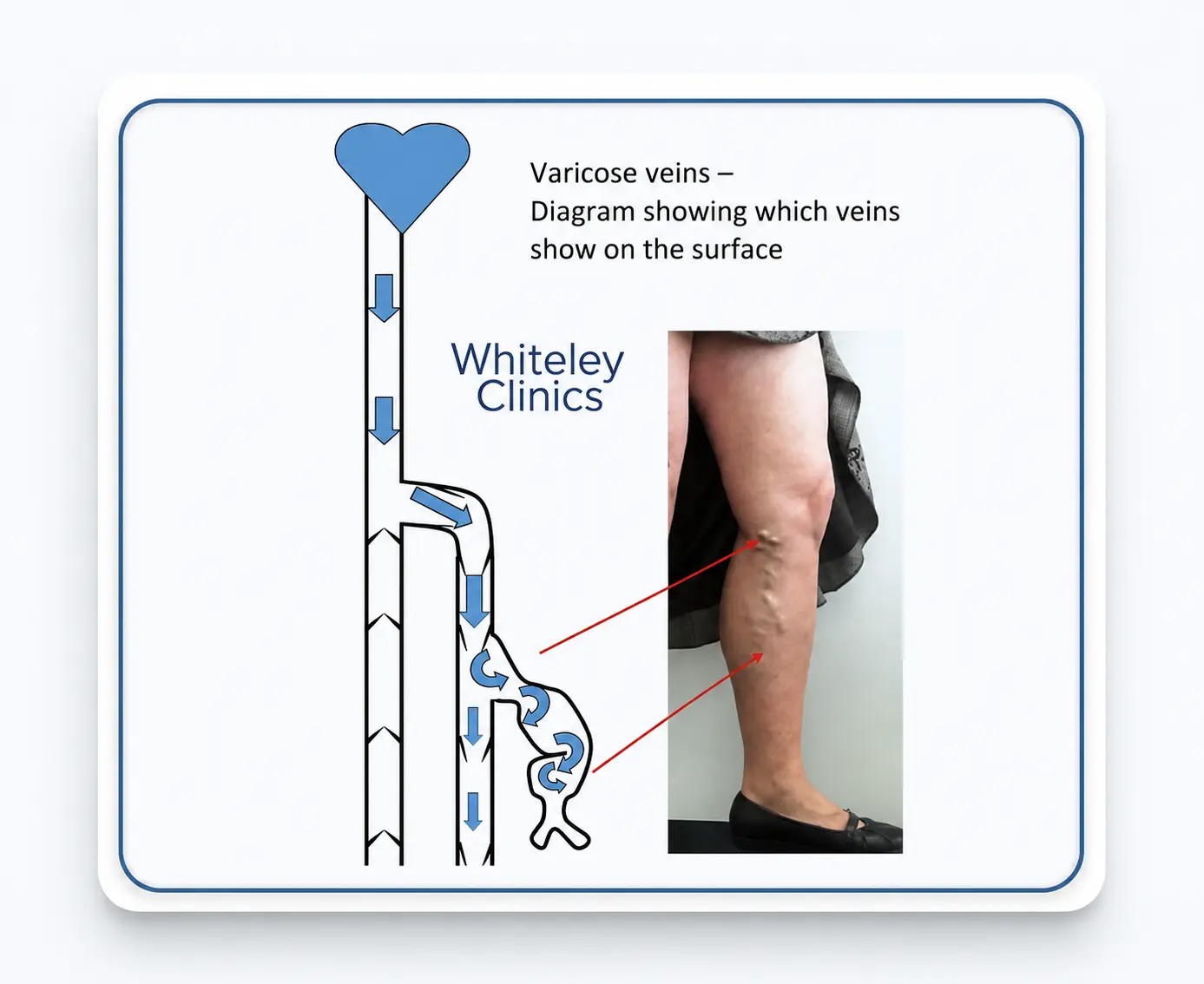
The veins that can become visible on the skin belong to Network Three (N3). These veins sit within Anatomical Compartment Three (AC3). When they enlarge and become tortuous, they appear as visible varicose veins.
This distinction explains why significant venous disease can exist without any obvious surface changes.
What Causes Hidden Varicose Veins?
The most common cause is venous reflux.
Healthy veins contain one-way valves that keep blood moving upwards towards the heart. When these valves become incompetent, blood falls back down the leg under the influence of gravity.
This reverse flow increases venous pressure. As pressure builds, blood begins to pool within the affected veins. The resulting venous hypertension triggers inflammation within surrounding tissues and gradually damages the skin and underlying structures.
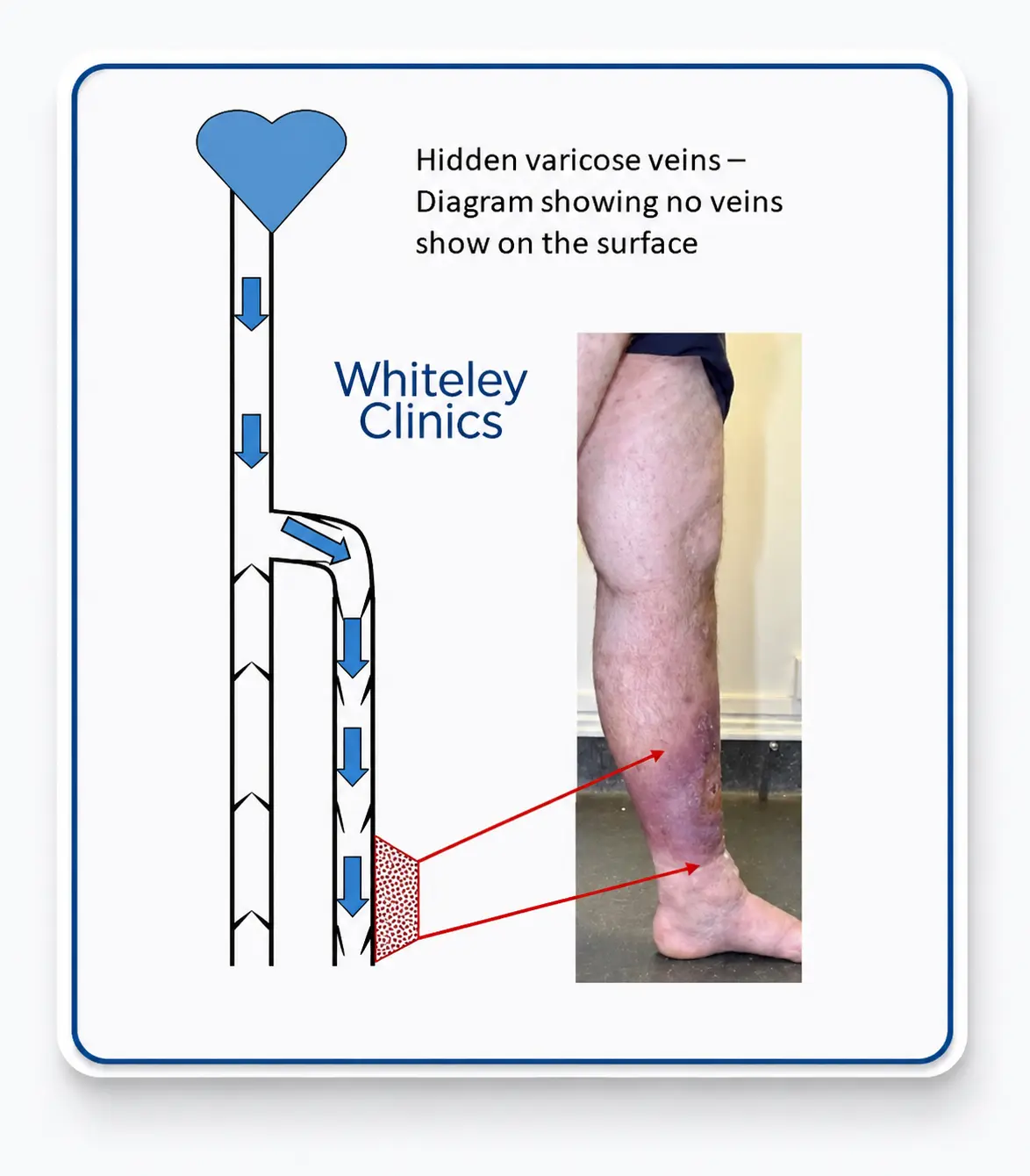
Visible varicose veins develop when reflux reaches the superficial veins within AC3. However, this condition occurs when reflux remains confined to the truncal veins within AC2.
Their hidden anatomical location means that venous disease may develop and progress despite the absence of any obvious varicose veins on the skin.
In fact, this pattern occurs in approximately 50% of people with venous disease.
Some people ask: Can I Have Varicose Veins I Can't See?
Yes.
Many people assume that varicose veins must be visible. However, venous reflux can develop within the truncal veins without affecting the superficial veins that sit closer to the skin.
As a result, blood flows abnormally within the venous system, yet no bulging veins appear on the surface.
This explains why some patients experience symptoms of venous disease despite having legs that appear completely normal.
Consequently, venous disease may still be present even when no visible veins are seen on the surface.
A frequent concern among patients is why their legs hurt when no varicose veins are visible?
Increased pressure within the veins is the key factor behind these symptoms.
When blood pools within incompetent veins, pressure rises throughout the lower limb. This pressure affects the tissues, microcirculation, and inflammatory pathways surrounding the veins.
Consequently, symptoms can develop long before visible varicose veins appear.
Pain, aching, heaviness, and fatigue are often signs of underlying venous dysfunction rather than visible vein enlargement. Therefore, symptoms should never be dismissed simply because the skin appears normal.
What Does It Feel Like to Have Hidden Varicose Veins?
The clinical presentation of this condition is very similar to the symptoms observed in patients with visible varicose veins.
Common symptoms and signs include:
- Aching legs, particularly when standing
- Heavy legs
- Tired or fatigued legs
- Tenderness in the legs
- Thread veins or spider veins
- Swollen ankles
- Venous eczema around the ankles
- Brown skin staining caused by haemosiderin deposition
- Venous leg ulcers
- Superficial thrombophlebitis (phlebitis)
Symptoms often worsen after prolonged standing and may gradually become more severe if the underlying reflux remains untreated.
How Hidden Varicose Veins Can Progress
Hidden varicose veins are not simply a cosmetic issue.
When venous reflux remains uncontrolled, a chronic inflammatory process gradually develops around the ankle and lower leg. Over time, this ongoing inflammation may progress and contribute to the development of more advanced venous disease.
The earliest sign is often ankle oedema (CEAP C3). As venous hypertension persists, patients may develop venous eczema and skin pigmentation changes caused by haemosiderin deposits (CEAP C4).
Eventually, the skin can break down, resulting in venous leg ulcers (CEAP C6).
Early diagnosis can help prevent these complications and improve long-term outcomes.
Why a Duplex Ultrasound Scan Is Essential
A physical examination alone cannot reliably identify hidden varicose veins.
Even experienced doctors and nurses cannot confirm the absence of hidden venous disease without imaging.
A venous duplex ultrasound scan remains the gold standard investigation. The examination provides detailed information about blood flow within the veins, helping specialists detect reflux, evaluate valve competence, and pinpoint the source of the problem.
Importantly, duplex ultrasound can also identify incompetent perforator veins and other less common causes of reflux that may contribute to symptoms or recurrent venous disease.
Without duplex ultrasound, this condition may remain undiagnosed.
The Importance of Incompetent Perforator Veins
These perforating veins act as a link between the superficial venous network and the deep venous system.
When they lose competence, they permit abnormal bidirectional or reversed blood flow between these two systems. Evidence indicates that incompetent perforator veins are linked to recurrent varicose veins as well as persistent venous symptoms.
They are also acknowledged as a significant factor contributing to treatment failure when they are overlooked or inadequately managed.
Therefore, a thorough venous evaluation should always incorporate an assessment of perforator vein function.
How Common Are Hidden Varicose Veins?
Visible varicose veins affect approximately 15% to 20% of adults.
However, a similar proportion of adults also have hidden varicose veins.
These figures suggest that venous reflux disease is far more common than many people realise.
As awareness increases, more patients are receiving accurate diagnoses for symptoms that were previously attributed to other causes.
A Brief History of Hidden Varicose Veins
The concept of hidden venous disease is not new.
Medical literature discussed hidden perforator veins as early as 1970. However, clinicians at that time did not have access to modern duplex ultrasound technology and therefore could not fully understand the complexity of venous reflux patterns.
Advances in venous imaging have since transformed the diagnosis and treatment of hidden varicose veins, allowing specialists to identify reflux that would previously have remained undetected.
Why Early Diagnosis Matters
Hidden varicose veins can cause significant symptoms despite the absence of visible varicose veins. Left untreated, the condition may progressively worsen.
Evidence suggests that approximately one in twenty patients experiences deterioration each year when underlying venous reflux remains untreated.
For anyone experiencing persistent leg symptoms, a comprehensive venous duplex ultrasound assessment is the most reliable way to determine whether this condition is present.
Early diagnosis provides the opportunity to treat the underlying cause before more serious complications develop.