



Can Microsclerotherapy Effectively Remove Spider Veins?
July 18, 2026
Varicose veins occur because the valves inside the veins themselves, or more commonly the underlying veins, fail allowing blood to fall the wrong way down the veins on standing. This backward flow of blood or “venous reflux” causes a column of blood to push on the veins, making the walls bulge and become varicose.
Although, in the early stages of varicose vein formation there may be few or no symptoms, the development of varicose veins is often associated with some discomfort or aching. Surprisingly, symptoms are not related to how bad the varicose veins appear. In many patients, the smallest varicose veins can be very tense and symptomatic. Sometimes very large ones that are not under much pressure and hence do not have much in the way of wall tension, may not cause much in the way of symptoms, particularly in the short term.
Usually what happens is that varicose veins appear due to the vein itself dilating. This is called phase 1 passive reflux in the book understanding venous reflux the cause of varicose veins and venous leg ulcers (see: Understanding Venous Reflux book). As time passes and more valves give way in the veins, phase 2 passive reflux or active reflux develop increasing the pressure inside the veins, increasing wall tension and starting to cause symptoms. These symptoms may be due to wall tension in the vein, inflammation around the wall of the vein or even clots forming in the varicose veins (superficial venous thrombophlebitis or “phlebitis“).
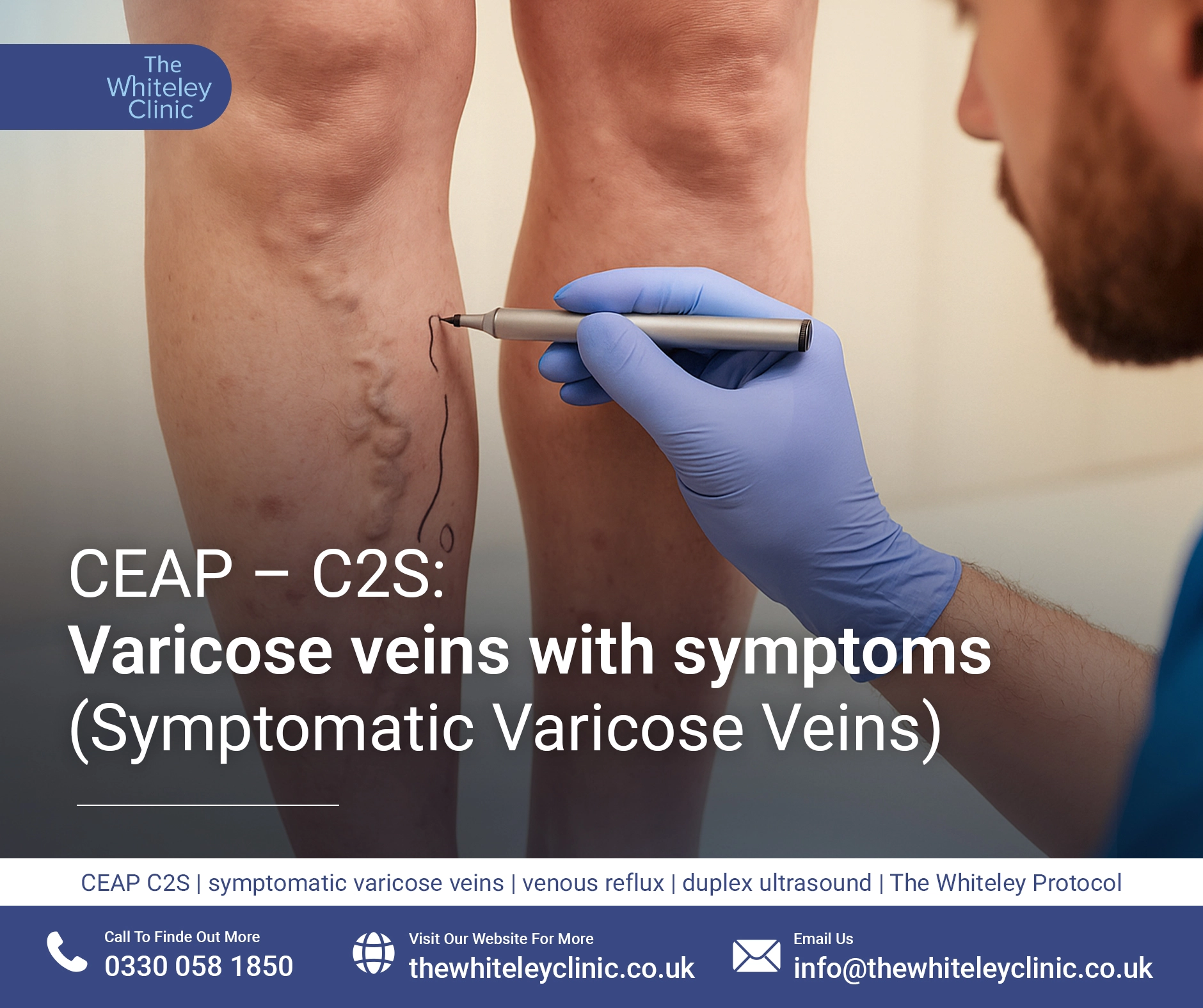
Symptomatic varicose veins (CEAP C2S) look exactly the same as asymptomatic varicose veins (CEAP C2A) to the observer as the only difference between the two is whether the patient feels any symptoms or not.
There is really very little medical difference between the two conditions as the risk of deterioration and complication, and hence threat to health is related to the pattern of the venous reflux itself and not whether the patient says that they can feel any discomfort or not. In addition, many patients who think they are asymptomatic have merely got used to the discomfort of the varicose veins, or do not put the symptoms down to being caused by the varicose veins. This becomes evident when the varicose veins are treated successfully for cosmetic reasons and the patient suddenly realise that their legs feel less tender, less heavy and often “lighter”.
Therefore the presence or absence of symptoms is more related to criteria used by the funders of healthcare as to who should be referred for varicose vein treatments and who will be funded by private medical insurance or government health care systems.
It is interesting to note that the complications of varicose veins and venous reflux disease are related to swelling, clot formation, bleeding, skin damage and leg ulcers, not to any symptoms such as tenderness or pain. Therefore, if we were being strictly scientific, symptoms will be virtually irrelevant in assessing varicose veins. However for generations, patients have been refused varicose vein treatment if their varicose veins are not painful because it seems logical to patients that if something doesn’t hurt, it isn’t serious. Of course a little thought shows that this is ridiculous. It is very rare that breast cancer, cervical cancer, aortic aneurysms, cataracts and a multitude of other very serious conditions cause pain – but most people would agree they need treatment to prevent the consequences of leaving them alone.
However, in the world of varicose veins, because so many people suffer from this problem, medical insurance and governments that fund healthcare use the perception that varicose veins are only serious if they are painful, as a reason to refuse funding for varicose vein treatments and because it appears logical superficially, patients accept it.
So, what symptoms are usually found in symptomatic varicose veins? The National Institute of Health Clinical Excellence Clinical Guidelines 168 (NICE CG 168) written in July 2013 state that the “typical” troublesome lower limb symptoms associated with varicose veins are:
It is one of the inconsistencies of the NICE Guidelines and that “swelling” is included as a “symptom”. If there is swelling this is venous oedema we should actually make the classification CEAP C3. In addition swelling is a sign that can be seen, not a symptom that is felt. However this is what is written in the guidelines.
As with asymptomatic varicose veins CEAP C2A, the underlying cause of varicose veins is almost always venous reflux.
In early varicose veins, it might just be that they are seen on the surface and those immediately associated with them. However, it is much more likely that the reflux has progressed deeper inside the leg, and venous reflux causing the varicose veins is coming from underlying incompetent veins. These are usually the great saphenous vein, anterior accessory saphenous vein, small saphenous vein, incompetent perforators or pelvic varicose veins.
As with all varicose veins, every individual has their own pattern of venous reflux and in a majority of cases, if proper in-depth venous duplex ultrasonography is performed by specialist vascular scientists, there is often more than one cause of the venous reflux. Failure to identify all of the causes and treat them is a major cause of recurrent varicose veins in the future.
If you do have symptomatic varicose veins (CEAP C2S), then it is sensible to have them investigated and treated. As with any medical condition, it is your own choice as to whether you want to seek treatment. However varicose veins will always deteriorate with time and more importantly, if you are already getting symptoms, treatment is required to relieve the symptoms.
Although in the past doctors have argued as to whether surgical treatment is needed or whether treatment with support stockings will suffice, a randomised controlled study was performed in (reactive study) which showed a clear improvement in quality-of-life at two years in patients who had had varicose veins treated surgically rather than those consigned to support stockings only.
Up until July 2013, patients were often told by general practitioners or medical insurance companies that they had to wear support stockings for six months before any treatment would be considered. This was shown to be nonsense by the above study and the NICE guidelines (CG 168) stated quite clearly that support stockings should not be used as a treatment for symptomatic varicose veins and patients should be referred for investigation and treatment at a vascular service that uses a multidisciplinary team to investigate and treat patients – just as has been recommended and performed by The Whiteley Clinic since 1999.
To get the correct treatment for symptomatic varicose veins, it is essential to have a specialised venous duplex ultrasound scan performed by a highly qualified vascular scientist to find out exactly what pattern of venous reflux is causing the problem and to identify all of the underlying venous reflux. It is not sufficient for a Dr to perform their own “quick scan” where they may identify a major cause of the venous reflux. It is essential for good treatment that all the different causes of venous reflux are identified and appropriate treatment courses recommended. This is the basis of The Whiteley Protocol® approach.
Once you have had in-depth venous duplex ultrasonography and all of the causes of the venous reflux causing the symptomatic varicose veins have been identified, your The Whiteley Clinic consultant will be able to discuss with you the optimal tailored approach to treating your venous reflux, to give you the best possible outcome and the lowest possible chance of recurrence in the future.